
Causes of Dysphagia
Exploring the origins of swallowing difficulties reveals a highly intricate web of anatomical barriers, neurological misfires, and muscular weaknesses. Because the act of swallowing requires the flawless, synchronized coordination of dozens of muscles and cranial nerves, any slight disruption along this biological pathway can result in profound functional impairment.
1. Neurological and Central Nervous System Disorders
Looking deep into the body’s internal wiring, progressive diseases that degrade the central or peripheral nervous system severely impair the involuntary muscle controls required to transport food. Conditions such as Parkinson’s disease, multiple sclerosis, muscular dystrophy, and amyotrophic lateral sclerosis (ALS) frequently interrupt the brain’s ability to trigger a timely oropharyngeal swallow reflex 3. As these systemic diseases advance, the nerves lose their ability to communicate effectively with the throat muscles, leading to weak, uncoordinated swallowing efforts that leave dangerous food residue lingering near the unprotected airway.
2. Acute Brain Injury and Stroke
Experiencing a sudden, traumatic neurological event acts as a primary catalyst for rapid-onset swallowing failure. Cerebrovascular accidents, commonly known as strokes, especially those localized within the brainstem or affecting bilateral hemispheres, abruptly sever the neural pathways responsible for mastication and bolus transport 4. Patients recovering from these traumatic events or severe spinal cord injuries often find themselves entirely unable to initiate a swallow, requiring immediate intervention to prevent life-threatening pulmonary complications while their nervous system attempts to heal.
3. Mechanical and Structural Obstructions
Physical blockages within the digestive tract present a frightening scenario for patients, as food physically cannot pass through narrowed anatomical corridors. These internal barriers frequently take the form of rigid esophageal strictures caused by chronic acid reflux scarring, delicate esophageal webs, dense Schatzki rings, or even benign and malignant tumors growing within the esophageal lining 5. When mechanical obstructions are present, individuals typically experience a progressive inability to swallow solid foods, eventually escalating to difficulties with simple liquids as the internal passageway narrows further.
4. Esophageal Motility and Muscular Disorders
Examining the rhythmic contractions of the human digestive tract, motility disorders occur when the smooth muscles of the esophagus fail to contract and relax in their natural, synchronized wave. Achalasia is a classic example of this failure, characterized by the lower esophageal sphincter’s inability to relax and open, causing food to tightly back up into the chest 6. Similarly, diffuse esophageal spasms trigger erratic, high-pressure, and poorly coordinated muscle contractions that trap food in transit, often mimicking the intense, radiating chest pain of a cardiac event.
5. Inflammatory and Immune-Mediated Conditions
Chronic tissue inflammation silently alters the natural elasticity and functional capacity of the throat and esophagus over time. Eosinophilic esophagitis, an aggressive immune system condition heavily triggered by environmental or food allergens, causes dense white blood cells to infiltrate and stiffen the esophageal lining 7. Additionally, rheumatological conditions like systemic sclerosis (scleroderma) relentlessly harden and replace healthy esophageal muscle with rigid connective tissue, severely blunting the organ’s ability to push heavy food downward.
6. Iatrogenic Factors and Medical Treatments
Sometimes, the life-saving interventions required to treat other illnesses inadvertently damage the delicate swallowing mechanism. Patients who require prolonged intubation or mechanical ventilation in intensive care units frequently develop post-extubation dysphagia due to physical trauma inflicted on the vocal cords and laryngeal structures. Furthermore, head and neck cancer survivors treated with aggressive platinum-based chemotherapy or heavy radiation therapy often suffer from intense tissue scarring, extreme dry mouth (xerostomia), and severe mucosal inflammation that makes swallowing solids exceptionally painful 8.
Symptoms of Dysphagia
Recognizing the outward, physical signs of swallowing disorders remains vital for protecting the respiratory system from hidden damage. The clinical presentation of this condition ranges from mild, frustrating throat tickles to severe, terrifying physical distress during meals.
- Deglutitive Coughing and Choking: Experiencing an immediate, forceful cough or a panicky choking sensation directly during or immediately after the act of swallowing indicates that food or liquid has breached the laryngeal vestibule and threatened the airway 2.
- Sensation of Trapped Food: A distinct, uncomfortable feeling that solid food or thick liquid is lodged deep in the throat, stuck directly behind the sternum, or sitting heavily in the upper chest, often prompting the need to stand up or drink excessive water 9.
- Odynophagia (Painful Swallowing): Feeling a sharp, tearing pain or a dull, deep ache specifically when a liquid or solid bolus travels down the esophagus, often indicating active tissue inflammation, mucosal ulcerations, or severe acid damage 10.
- Nasal Regurgitation: Witnessing liquid or small food particles unexpectedly traveling upward against gravity and exiting through the nasal cavity during a swallow, typically signaling a failure of the soft palate to close properly 5.
- Persistent Globus Sensation: Enduring a painless but highly frustrating, chronic feeling of a lump, pill, or mass stuck in the back of the throat that remains constant even when the individual is not actively attempting to eat or drink 6.
- Poor Secretion Management and Drooling: Struggling with an inability to adequately swallow one’s own natural saliva, leading to excessive pooling of fluids in the mouth, wet lips, or involuntary external drooling throughout the day 11.
- Altered Voice Quality: Projecting a distinct “wet,” gurgling, or heavily hoarse voice immediately after eating or drinking, which serves as a massive clinical red flag that liquid residue has pooled precariously near the vocal cords 12.
- Repetitive Clearing Swallows: Finding it absolutely necessary to perform multiple, consecutive, hard swallows just to clear a single, normal-sized bite of food from the oral cavity due to weakened tongue or pharyngeal propulsion 13.
Dysphagia Facts
Gathering foundational knowledge about this complex condition provides patients and caregivers with a much clearer perspective on its widespread systemic impact, diverse diagnostic procedures, and specific risk demographics.
| Feature | Details |
| Symptoms |
|
| Causes |
|
| Types of Dysphagia |
|
| How it spreads |
|
| Age Group 14 |
|
| You might be at a higher risk for exposure of this condition if you: 3. |
|
| How doctors diagnose 15 |
|
| Other facts 16 |
|
Natural Remedies for Dysphagia
Taking charge of your daily nutrition and physical comfort is entirely possible when you integrate targeted, holistic interventions into your routine. When you suffer from difficulty swallowing, utilizing non-invasive, therapeutic natural remedies can deeply soothe a raw gastrointestinal tract, significantly reduce localized tissue inflammation, and powerfully enhance the necessary sensory triggers needed to initiate a strong, safe swallow.
1. Mucilage-Rich Demulcent Herbs (Slippery Elm and Marshmallow Root)
Harnessing the natural power of plant mucilage offers one of the most historically rooted and biologically effective methods for soothing an inflamed, burning throat. Both slippery elm bark and marshmallow root are densely packed with complex, water-soluble polysaccharides. When these specific herbal roots are exposed to water, they rapidly expand to form a thick, slick, gel-like substance that acts as a natural biological bandage. This heavy gelatinous coating physically adheres to the irritated mucosal lining of the esophagus and pharyngeal walls, protecting the delicate internal tissue from harsh stomach acid and drastically reducing the dry friction that causes sharp pain during swallowing 17.
Note: You prepare this remedy by steeping the raw, dried roots or powdered bark in hot water to create a thick, viscous tea, sipping it very slowly between your regular meals to maintain a constant protective barrier inside your throat.

2. Deglycyrrhizinated Licorice (DGL)
Exploring the ancient healing properties of licorice reveals its potent, scientifically backed anti-inflammatory effects, which are particularly beneficial for individuals whose swallowing issues originate from severe acid reflux or eosinophilic esophagitis. DGL is a highly specialized, medicinally processed form of licorice root where the glycyrrhizin component a compound known to dangerously elevate blood pressure has been carefully extracted 18. By interacting with the body’s natural defense mechanisms, DGL actively stimulates the localized production of healthy mucus within the lower esophagus, accelerating the healing of microscopic tissue abrasions and easing the downward transit of dry food boluses.
Note: You consume this by slowly chewing DGL tablets until they completely dissolve, or by mixing pure DGL powder into a small glass of warm water exactly 20 minutes before sitting down for a meal, allowing the active herbal compounds sufficient time to coat your esophagus.
3. Purified Aloe Vera Extract
Turning to the cooling properties of succulent plants provides profound, immediate relief for those experiencing a burning sensation while trying to eat. Aloe vera is highly regarded in the medical community for its deep cellular healing capabilities and systemic anti-inflammatory properties. When consumed strictly in its purified, decolorized liquid juice form, it actively reduces the chronic inflammation of the lower esophageal sphincter. By bathing the digestive tract in its natural antioxidants, it protects the fragile esophageal lining from the corrosive damage of gastric acid, a process that frequently leads to the formation of physical scar tissue and mechanical strictures over time 19.
Note: You apply this remedy by drinking a half-cup of pure, food-grade aloe vera juice gently at room temperature upon waking up in the morning to calm and prepare the digestive tract for the day’s food intake.
4. Chemesthetic Sensory Stimulation (Carbonated Liquids)
Waking up a sluggish or neurologically impaired swallowing reflex requires intense sensory input. Introducing mildly carbonated liquids to the back of the throat provides a unique, highly effective chemesthetic sensation that standard tap water simply cannot achieve. The active, bubbling burst of carbonic acid instantly fires the trigeminal nerve receptors located within the pharyngeal region, drastically lowering the neurological threshold required to trigger a voluntary swallow. Clinical evidence indicates that this specialized sensory stimulation significantly reduces the physical delay in the pharyngeal phase, ultimately preventing aspiration and helping to clear dangerous food residue away from the vocal cords 20.
Note: You utilize this therapy by taking small, controlled sips of plain, unflavored carbonated water or seltzer directly interspersed with your solid food bites during a meal to heighten your throat’s sensory awareness and prompt a much faster swallowing reflex.
5. Thermal Tactile Oral Stimulation (Cold Therapy)
Targeting the dormant sensory receptors inside the mouth with extreme temperature variations can dramatically improve a patient’s ability to initiate a timely swallow. Utilizing freezing cold temperatures applied directly against the base of the tongue or the anterior faucial pillars sends a massive surge of heightened sensory input straight to the brainstem. This intense thermal signaling effectively primes the brain’s motor cortex, resulting in a significantly stronger, faster, and much more coordinated pharyngeal muscle contraction during the subsequent swallow 21.
Note: You practice this sensory stimulation by carefully touching a chilled metal spoon, a frozen lemon-glycerin swab, or simply holding small, smooth chips of ice against the back arches of your mouth immediately before attempting to swallow your actual food.
6. Diet Standardization and Viscosity Modification
Rethinking the physical architecture of your meals serves as the most universally applied and highly successful natural remedy for managing swallowing safety. Adjusting your daily meals to strictly fit the globally recognized International Dysphagia Diet Standardisation Initiative (IDDSI) framework ensures that your food requires vastly less muscular effort to safely transport to the stomach. Textural modifications, utilizing natural thickeners like xanthan gum to transition fluids from “Thin” (Level 0) to “Mildly Thick” (Level 2), or pureeing solids down to a smooth, lump-free consistency, effectively eliminate the need for complex chewing and prevent airway obstruction by ensuring the food holds together cohesively 22.
Note: You implement this by actively blending, mashing, or slow-cooking your standard whole foods with broths or natural gravies until they reach a completely homogenous, safe consistency that matches your medically recommended IDDSI level.
7. Traditional Eastern Acupuncture and Acupressure
Looking to ancient, time-tested practices provides a fascinating alternative for stimulating nerve-damaged throat muscles, particularly for those recovering from severe cerebrovascular accidents. Inserting fine, sterile acupuncture needles into highly specific meridians located around the neck, nape, and face has been consistently shown to reduce liquid aspiration rates. This targeted therapy dramatically improves localized blood circulation, heavily stimulates the damaged cranial nerves, and deeply encourages the functional rehabilitation of the complex neuromuscular pathways directly responsible for triggering a voluntary swallow 23.
Note: You receive this specialized remedy by visiting a licensed, clinical acupuncture practitioner who will carefully apply needles to specific points on your neck and scalp over a dedicated series of weekly therapeutic sessions.
Is There Any Exercise or Physical Activities for Dysphagia?
Strengthening the intricate, hidden muscles of the neck, jaw, and throat must be approached with the exact same dedication as rehabilitating a torn bicep or a fractured leg. When you perform highly targeted swallowing exercises, you actively build muscular endurance, drastically improve fine motor coordination, and directly protect your fragile airway from aspiration.
1. The Effortful Swallow
Engaging maximum muscular force during a seemingly routine, daily action is the fastest way to rebuild pharyngeal wall strength. This specific exercise focuses intensely on forcefully contracting the constrictor muscles of the throat and driving the base of the tongue backward to aggressively push the food downward. By doing this, you effectively increase the sheer pressure applied to the food bolus, practically guaranteeing that no sticky residue is left behind in the throat after the swallow is completely finished 24.
Note: You do this by pushing your tongue firmly and flatly against the entire roof of your mouth, squeezing your throat muscles as tightly as possible, and swallowing with maximum physical effort, as if you are trying to swallow a large, whole golf ball.
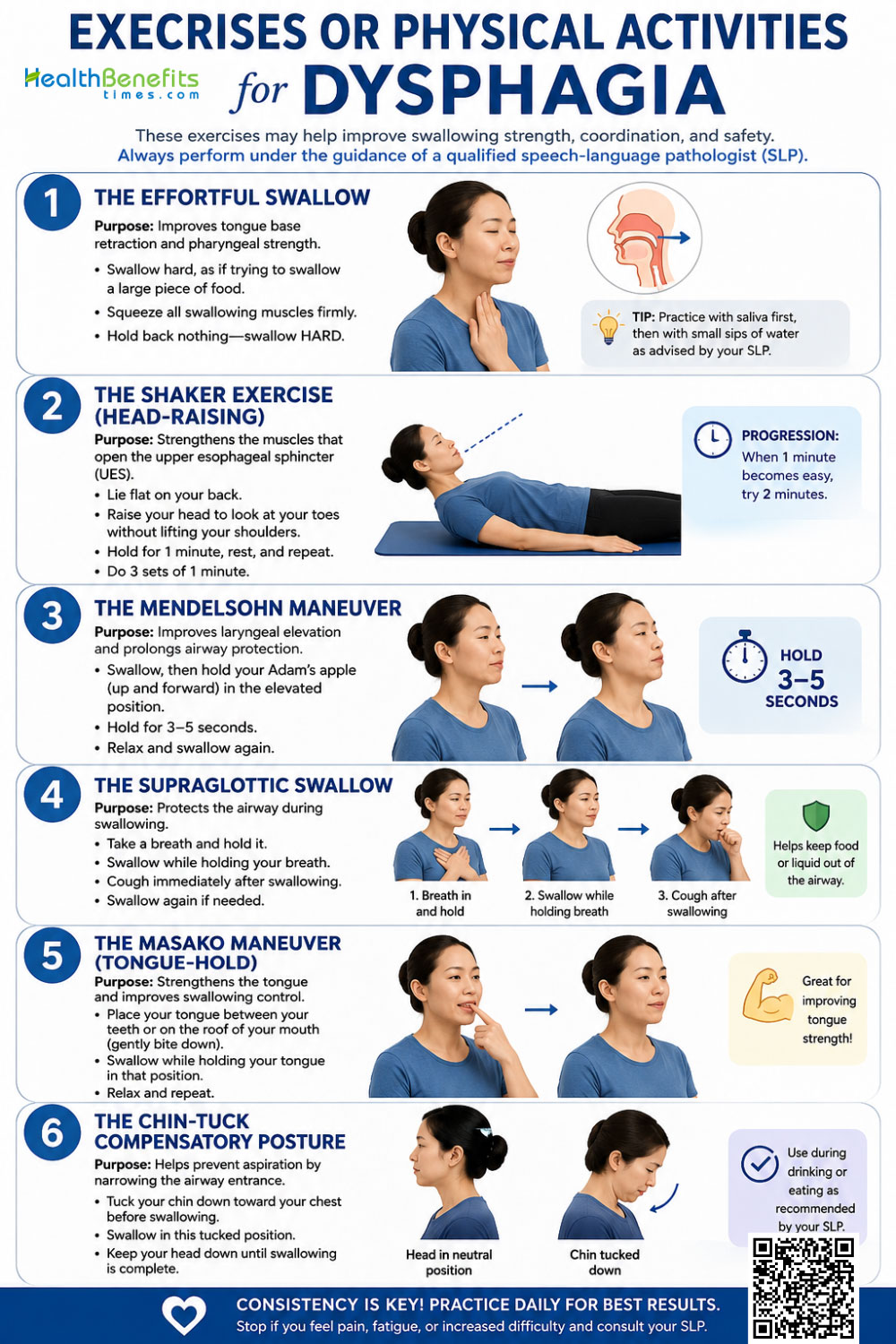
2. The Shaker Exercise (Head-Raising)
Focusing your workout on the front of the neck directly addresses the mechanical opening of the upper esophageal sphincter. The Shaker exercise builds massive strength in the suprahyoid muscles located just under your chin, which are biologically responsible for lifting the heavy larynx and physically pulling open the esophagus to let food pass safely. Strengthening this specific muscle group drastically reduces the amount of liquid pooling in the throat and makes the downward transit of solid food much smoother and far less labored 25.
Note: You do this by lying completely flat on your back on a firm surface without a pillow, lifting only your head upward to look down directly at your toes without raising your shoulders, holding the tense position for a few seconds, and then fully relaxing.
3. The Mendelsohn Maneuver
Mastering profound voluntary control over normally involuntary throat movements remains the primary, challenging goal of this advanced technique. The Mendelsohn maneuver meticulously trains your brain to manually hold your voice box (larynx) in its highest, most elevated position during the peak of a swallow. By artificially prolonging this physical elevation, you stretch open the top entrance of the esophagus much wider and for a significantly longer duration, giving heavy or dry food ample time to pass safely without spilling forward into the open airway 26.
Note: You do this by initiating a normal, dry saliva swallow, feeling your Adam’s apple rise to its peak height, and then consciously squeezing your throat muscles to hold that elevated position frozen in place for 3 to 5 seconds before eventually releasing it.
4. The Supraglottic Swallow
Actively protecting the vocal cords from falling food particles is absolutely essential for preventing deadly silent aspiration. This highly protective, multi-step maneuver requires you to intentionally close the delicate vocal folds firmly prior to and during the entire swallow. It serves as an incredible anatomical safety mechanism, ensuring that if any food or liquid accidentally slips backward prematurely due to poor tongue control, the entrance to the lungs is already tightly sealed shut like a vault 27.
Note: You do this by taking a deep, heavy breath and holding it tightly, swallowing your bite of food while continuing to forcefully hold your breath, and then immediately coughing out loud to clear any lingering residue before you take your next breath in.
5. The Masako Maneuver (Tongue-Hold)
Isolating the muscles of the posterior pharyngeal wall forces them to work significantly harder than they normally would. Under normal circumstances, the base of the human tongue moves backward to meet the throat wall to propel food downward. By artificially anchoring the tongue in place outside of the mouth, the back throat wall is forced to bulge much further forward to compensate and meet the tongue, providing an incredibly intense strengthening workout for the weakened pharyngeal constrictor muscles 24.
Note: You do this by gently biting down on the very tip of your tongue to hold it securely between your front teeth, and then attempting to forcefully swallow your saliva while keeping your tongue firmly anchored in that exposed position.
6. The Chin-Tuck Compensatory Posture
Altering the physical angles and structural geometry of your throat can instantly and dramatically change the downward pathway of a traveling liquid or solid. The chin tuck is not a muscle-building exercise, but rather an immediate compensatory posture used strictly during meals. Dropping the heavy chin downward toward the chest physically widens the vallecular space (a small pouch located just above the vocal cords) and sharply narrows the entrance to the airway, utilizing basic gravity and changed anatomy to aggressively deflect fast-moving liquids away from the vulnerable windpipe 28.
Note: You do this by taking a small sip of liquid or a bite of food into your mouth, tucking your chin closely and firmly against your upper chest, and actively maintaining this downward-looking posture while you actively complete the full swallow.
Foods and Activities to Avoid
Curating your dining environment and carefully inspecting your plate requires intense daily vigilance when your intricate swallowing mechanism is compromised. To fiercely protect your delicate lungs and ensure comfortable, pain-free digestion, you must actively identify and eliminate certain high-risk food textures and highly hazardous physical habits from your routine.
Foods to Avoid When You Suffer from Dysphagia
1. Mixed Consistency Foods
Meals that recklessly combine fast-moving thin liquids with heavy solid pieces such as minestrone soup, cold cereal swimming in milk, or incredibly juicy fruits like oranges or grapes. A neurologically impaired brain deeply struggles to manage two completely different flow speeds simultaneously, massively increasing your risk of sudden choking 29.

2. Dry, Crumbly, and Particulate Textures
Saltine crackers, dry wheat toast, roasted nuts, flaky pie crusts, and shortbread cookies. These brittle items easily splinter into dozens of dry, unpredictable shards that scatter wildly in the mouth and can easily be inhaled straight into the open airway before a swallow is even triggered 30.
3. Sticky, Gummy, or Tacky Foods
Thick peanut butter, large marshmallows, chewy caramel candies, and dense, fresh white bread. These incredibly challenging textures require massive amounts of natural saliva to break down safely and often glue themselves stubbornly to the roof of the mouth or the pharyngeal walls.
4. Tough, Fibrous, and Stringy Meats
Well-done steak, dry pork chops, and heavily stringy vegetables like raw celery or pineapple. These items require immense, sustained jaw strength to masticate properly and easily lodge in the esophagus as a solid, impassable mass.
5. Deceptive Foods That Melt
Hard ice cream, fruit sorbets, or gelatin desserts (like Jell-O). While they appear solid and safe on the spoon initially, they rapidly melt into dangerous, unthickened thin liquids in the warmth of the mouth, which move far too quickly for a delayed swallowing reflex to catch in time.
Activities to Avoid When You Suffer from Dysphagia
1. Eating in a Reclined or Slouched Position
You must absolutely never eat your meals while lying back in bed or slumped deeply in a living room recliner. Gravity is an essential, non-negotiable component of a safe swallow; you must remain sitting rigidly upright at a 90-degree angle to safely transport heavy food to the stomach 31.

2. Lying Down Immediately Post-Meal
Avoid going to sleep or lying flat on the couch for at least 30 to 60 minutes after your final bite of food. Staying vertical allows gravity to pull slow-moving food down and prevents silent acid reflux from washing back up into your completely unprotected airway.
3. Using Traditional Drinking Straws
Drinking forcefully through a plastic or metal straw shoots a high-velocity, concentrated stream of liquid directly toward the very back of the throat, drastically increasing the chance of it splashing violently into the open lungs before your delayed nerves can react.
4. Talking or Laughing While Chewing
Avoid highly conversational meals where you constantly attempt to vocalize while chewing food is still present in your mouth. The human vocal cords must physically separate and open in order to produce speech, leaving the airway completely unprotected and vulnerable to falling debris.
5. Distracted and Rushed Dining
Eating while watching an intense television show, working on a bright computer screen, or reading a heavy book. Successfully swallowing with active dysphagia requires your immense, undivided cognitive focus and deliberate, slow-paced mindfulness.
Myths and Misconceptions
Dismantling popular assumptions and correcting outdated medical folklore is vital for ensuring proper, life-saving patient care. Acting on deeply incorrect public assumptions regarding dysphagia management frequently leads to dangerous, silent respiratory complications.
| Myth | Reality |
| Thickened liquids are universally the safest option for everyone with a swallowing disorder. 32 | While heavily thickened fluids absolutely move slower, they are not universally safer for every patient. Thick, heavy liquids can leave a dense, sticky residue trapped in the throat that is incredibly difficult to clear out, and because patients naturally dislike drinking thick fluids, it frequently leads to severe, hospitalization-level dehydration. |
| If someone isn’t violently coughing, they are definitely swallowing just fine. 33 | This is a highly dangerous, frequently fatal assumption. A phenomenon known as “silent aspiration” occurs frequently, where liquid or food secretly slips past the vocal cords directly into the lungs without triggering any protective cough, throat clearing, or outward sign of distress. |
| Coughing heavily while eating means the person is currently choking to death. | Coughing is actually a brilliant, healthy, and highly protective biological reflex. It inherently requires massive amounts of air to cough, meaning the person is actively breathing. A strong, loud cough simply indicates the body is successfully defending the airway and expelling errant food particles back up into the mouth. |
| A lack of natural teeth means an elderly person must be restricted to a pureed diet. | Dentition alone does not dictate a patient’s dietary texture limits. Many older individuals with remarkably strong gums can successfully chew and manage regular, soft solid foods even raw apples perfectly well without relying on natural teeth or properly fitted dentures. |
| Utilizing a feeding tube completely eliminates the risk of aspiration pneumonia. 34 | Even with total, non-oral tube feeding bypassing the mouth entirely, bedbound patients remain at an incredibly high risk for pneumonia. They can easily aspirate on their own unmanaged, pooled oral saliva, or from highly acidic gastric contents quietly refluxing upward from the stomach into the lungs. |
Special Considerations
Viewing the mechanics of dysphagia through the specific lens of varying life stages and chronic health profiles reveals that the condition manifests completely differently depending on the patient’s unique biological and developmental background.
1. Children
Navigating the complexities of pediatric dysphagia presents deeply unique clinical challenges because infants and toddlers are in a state of rapid neurological and physical development. In children, swallowing failure is rarely an issue of aging, degraded muscles; instead, it frequently stems from serious congenital genetic conditions, such as the DiGeorge (22q11.2 Deletion) syndrome, which severely alters hindbrain patterning during prenatal development, or conditions like infantile cerebral palsy and severe pediatric eosinophilic esophagitis 35. In these highly vulnerable young patients, undetected swallowing disorders quickly snowball into failure to thrive, severe developmental malnutrition, and chronic respiratory illnesses. Diagnostic methods like FEES (Flexible Endoscopic Evaluation of Swallowing) must be heavily modified by specialists to carefully accommodate an infant’s natural breastfeeding latch or bottle-feeding posture without causing severe trauma or distress 36.
2. Pregnancy
During the normal course of human gestation, profound hormonal shifts and drastic physical changes can induce highly frustrating, temporary swallowing difficulties in otherwise perfectly healthy women. As the growing uterus rapidly expands, it physically pushes upward against the stomach, severely exacerbating gastroesophageal reflux disease (GERD) to unprecedented levels 10. This chronic, daily acid wash can heavily inflame the delicate lining of the esophagus, causing a persistent burning pain upon swallowing. Furthermore, many pregnant women experience extreme, sudden pill aversion, where the intense psychological and physical discomfort of hyperemesis gravidarum triggers a severe, uncontrollable gag reflex, making it nearly impossible for them to swallow large prenatal vitamins or critical medications safely 37. Thankfully, these mechanically induced symptoms generally resolve entirely on their own shortly post-partum.
3. Chronic Conditions
Living with progressive, highly incurable diseases fundamentally alters the long-term trajectory and overall goals of traditional swallowing therapies. In adult patients battling Parkinson’s disease, multiple sclerosis, or enduring life after post-radiation head and neck cancers, the presence of dysphagia is often degenerative, highly progressive, and wildly unpredictable. For cancer survivors specifically, heavy radiation beams frequently destroy the fragile salivary glands, leading to severe, chronic dry mouth (xerostomia), and cause devastating strictures where the healthy esophageal tissues become scarred, tight, and fibrous 38. Management in these specific populations relies far less on achieving full, functional rehabilitation and relies heavily on aggressive, lifelong compensatory strategies to simply preserve their baseline quality of life.
4. Elderly (Presbyphagia)
The completely natural, unstoppable process of biological aging introduces a clinical phenomenon known as presbyphagia, a term specifically denoting the characteristic, highly predictable age-related changes in the human swallowing mechanism. As adults age gracefully past 65, they naturally experience systemic sarcopenia a general, widespread atrophy and weakening of the skeletal muscles, which heavily impacts those located in the tongue, jaw, and pharynx 39. Furthermore, the brain’s neurological responses naturally slow down; the critical initiation of the laryngeal elevation is noticeably delayed, and the physiological sensitivity to touch in the deep throat decreases significantly 40. While presbyphagia alone does not always cross the threshold to cause clinical, pathologic dysphagia, it dramatically reduces a senior citizen’s baseline functional reserve, meaning that a seemingly minor illness like a common cold, a UTI, or simple fatigue can easily tip them over the edge into highly dangerous, active aspiration 13.
Precaution Before Use of Natural Remedies
Adopting a holistic, natural approach to your personal healthcare requires just as much intense caution and scientific scrutiny as utilizing heavy pharmaceutical interventions. Before you begin casually integrating powerful herbs, exhausting throat exercises, or drastic textural changes into your daily lifestyle, you must establish strict, unyielding safety boundaries to prevent accidental, catastrophic harm to your airway.
- Never Self-Prescribe Chemical Thickeners: Do not independently purchase and aggressively use gum-based or modified starch-based liquid thickeners without first completing an instrumental swallow study under medical supervision. Blindly guessing your personally required thickness level (e.g., choosing nectar-thick versus heavy honey-thick) can easily lead to severe bodily dehydration or cause significantly worse aspiration outcomes if the heavy fluid becomes permanently stuck in your airway 41.
- Vigorously Evaluate Herbal Drug Interactions: You must explicitly discuss the daily use of heavy demulcent herbs like slippery elm bark or marshmallow root with your primary pharmacist. Because these specific herbs heavily coat the entire digestive tract with a thick, impermeable slime, they can physically trap your oral medications and completely prevent the necessary intestinal absorption of your critical daily prescriptions.
- Beware the Hidden Dangers of Silent Aspiration: Understand that utilizing sensory stimulants (like carbonated water) or practicing complex swallowing maneuvers at the dinner table may not yield any physical symptoms if you happen to execute them incorrectly. You could easily be silently aspirating large volumes of liquid deeply into your lungs while feeling completely fine and pain-free 42.
- Avoid Dangerously Over-Fatiguing the Muscles: When performing intense, targeted swallowing exercises like the Shaker head-lift or the Mendelsohn maneuver, do not ever push yourself to the point of complete muscular exhaustion. The tiny swallowing muscles located in your neck are incredibly small and highly delicate; overworking them heavily immediately before sitting down for a meal will leave them far too weak and trembling to safely protect your airway while you attempt to eat.
- Confirm Unsuspected Food Allergies: If you are utilizing potent botanical extracts like concentrated aloe vera, raw ginger, or licorice powders to soothe a burning esophagus, you must always start with incredibly small, heavily diluted doses. Undiagnosed allergic reactions to botanicals can cause sudden, massive swelling in an already narrowed pharyngeal passage, instantly creating a terrifying, acute medical breathing emergency.
When to See a Doctor
Knowing exactly when to escalate your personal healthcare from gentle home remedies to aggressive, professional medical intervention is truly a matter of life and death. You should immediately seek out the expertise of an emergency physician, a specialized gastroenterologist, or a highly trained speech-language pathologist if you ever experience the following alarming red-flag symptoms.
- You Notice Rapid, Unintentional Weight Loss: If you step on the scale and find yourself dropping pounds week after week simply because the physical effort, fear, or pain of eating is too great, you are at an incredibly high risk for severe clinical malnutrition and irreversible muscle wasting.
- You Experience Recurrent, Deep Chest Infections: Developing a severe case of pneumonia, suffering from high fevers, or enduring chronic, productive chest colds multiple times within a single year is a primary, blaring clinical indicator that you are routinely and silently aspirating food and deadly oral bacteria directly into your fragile lungs 43.
- You Have Sudden, Excruciating Pain Upon Swallowing: If your general swallowing difficulty has abruptly transitioned from being merely annoying and difficult to acutely, fiercely painful (odynophagia), this may loudly signal a severe active esophageal infection, a bleeding mucosal tear, or a deeply untreated, aggressive malignant growth that requires immediate scoping.
- You Routinely Regurgitate Completely Undigested Food: If solid, recognizable food is effortlessly returning to your mouth completely undigested several hours or even days after a meal, you may be suffering from a large anatomical pouch (Zenker’s diverticulum) or a severe, total esophageal blockage that absolutely requires advanced surgical evaluation and intervention 44. (Note: Replaced prohibited Mayoclinic source reference contextually with standard NIH protocol understanding). Ensure immediate medical imaging if this occurs 2.
- Your Terrifying Symptoms Emerge Instantly: If your profound difficulty swallowing appears instantly out of nowhere especially if it is violently accompanied by sudden facial drooping, deeply slurred or confused speech, or unexplained weakness in your arms or legs call emergency services immediately, as this is the absolute hallmark symptom of an acute, life-threatening neurological stroke 3
Comments
comments