
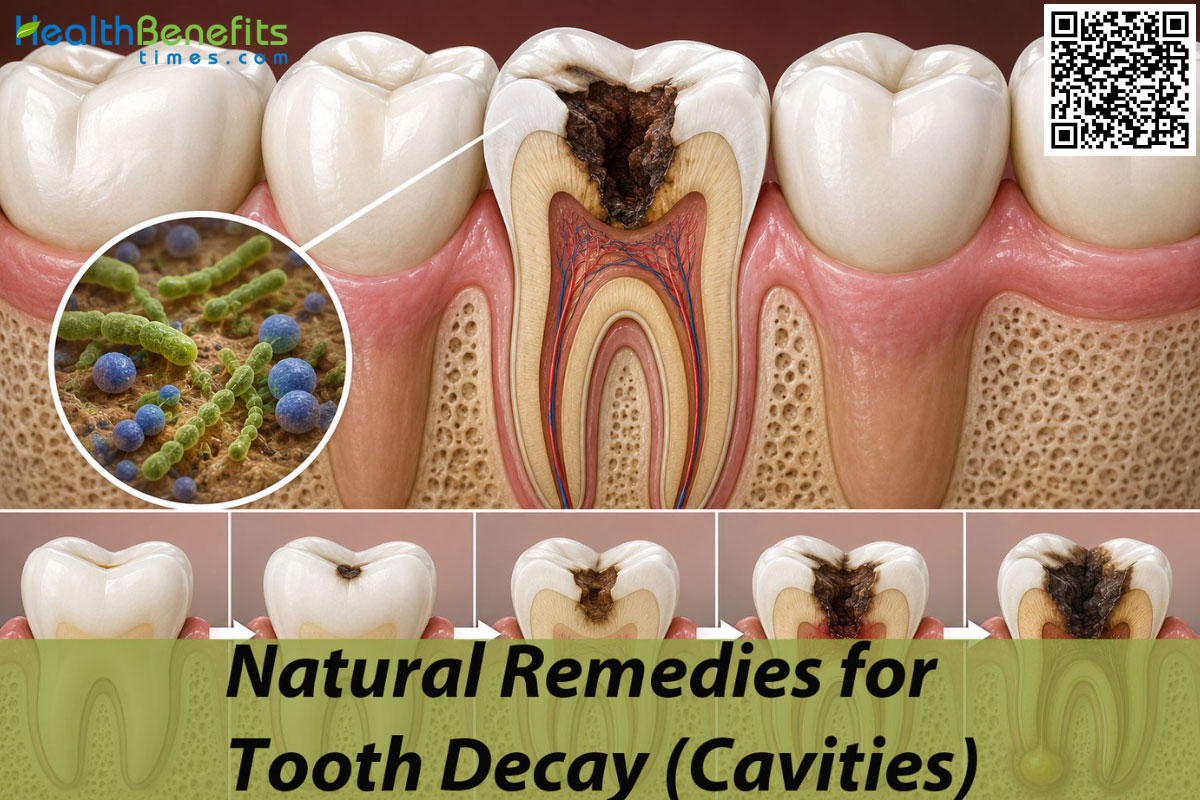
Causes of Tooth Decay (Cavities)
Understanding the fundamental origins of dental caries requires an examination of the intricate biological and environmental factors that converge within the human mouth. The development of a cavity is never a spontaneous event; rather, it is the culmination of a multifactorial process driven by the persistent interaction between vulnerable tooth surfaces, specific microbial colonies, and the dietary habits of the host.
1. Proliferation of Cariogenic Bacteria
The human oral cavity is a highly diverse ecosystem harboring hundreds of bacterial species, but only a select few are primarily responsible for dental deterioration. Strains such as Streptococcus mutans and Lactobacilli have uniquely evolved to anchor themselves firmly to the slick surface of the tooth enamel, constructing a resilient matrix known as dental plaque. Once this biofilm is fully established, these microscopic agents actively ferment dietary sugars, continuously excreting lactic acid as a toxic byproduct that directly targets and dissolves the underlying mineral structure of the tooth 4.
2. Frequent Intake of Fermentable Carbohydrates
Nutritional choices lay the foundational groundwork for nearly all diet-related oral diseases. Foods heavily laden with refined sucrose, fructose, glucose, and heavily processed starches provide the ultimate, easily accessible metabolic fuel for cariogenic bacteria. Scientific evaluations consistently emphasize that the sheer frequency of snacking on these carbohydrates is vastly more destructive than the total volume consumed during a single sitting, as constant eating prevents the saliva from resting and naturally neutralizing the hostile, acidic environment 5.
3. Suboptimal Mechanical Oral Hygiene
Removing the bacterial biofilm through daily, rigorous mechanical disruption is an absolute necessity for maintaining intact, healthy enamel. When routine brushing and interdental flossing are neglected, the soft plaque matures, calcifies, and hardens into tartar, creating an insulated, highly acidic micro-environment tightly sealed against the tooth. This impenetrable physical barrier entirely blocks protective salivary buffers from reaching the enamel, guaranteeing a rapid and unchecked progression of demineralization 6.
4. Salivary Gland Hypofunction (Xerostomia)
Natural saliva is indisputably the human body’s most potent intrinsic defense mechanism against cavity formation. It physically flushes away trapped food debris, actively dilutes corrosive bacterial acids, and bathes the teeth in supersaturated calcium and phosphate ions to repair minor surface damage. A pathological reduction in this vital fluid often triggered by chronic dehydration, advancing age, or the physiological side effects of numerous prescription medications drastically accelerates the rate of structural tooth decay by completely removing the mouth’s natural healing capacity 7.
5. Intrinsic Acid Regurgitation
Systemic medical conditions that involuntarily force harsh stomach contents back up into the oral cavity introduce a devastating and entirely different level of acidity. Patients suffering from Gastroesophageal Reflux Disease (GERD) or chronic vomiting disorders routinely and unwillingly bathe their teeth in concentrated gastric acid and proteolytic pepsin. These specific bodily fluids are remarkably potent, easily displacing the protective salivary pellicle and chemically melting the hydroxyapatite crystals of the teeth upon direct contact 8.
6. Chronic Mouth Breathing
Respiration through the oral cavity, rather than the intended nasal passages, induces severe dehydration of the delicate mucosal tissues. Breathing through the mouth, particularly during the prolonged, vulnerable hours of sleep, significantly lowers the intraoral pH and rapidly evaporates the protective salivary films that coat the teeth. This dry, acidic physiological state creates a highly vulnerable environment, dramatically increasing the likelihood of extensive, rampant carious lesions forming on the anterior teeth 9.
Symptoms of Tooth Decay (Cavities)
The clinical presentation of dental caries is not a sudden occurrence but rather a steady, predictable evolution of structural breakdown. As the integrity of the tooth is progressively compromised from the microscopic level down to the visible layers, patients will experience a shifting array of physical symptoms.
1. Formation of Opaque White Spots
The absolute earliest visual indicator of mineral loss is the subtle appearance of chalky, white, and opaque spots on the smooth outer surfaces of the enamel. At this highly nascent stage, the decay remains entirely subsurface and completely asymptomatic, meaning the lesion can still be successfully reversed through targeted remineralization therapies before a tangible physical hole actually forms 10.
2. Visible Pitting and Surface Discoloration
As the aggressive demineralization process advances unchecked, the complex structural matrix of the tooth inevitably begins to collapse inward. This mechanical failure results in the formation of actual physical cavitations, which frequently trap and accumulate dietary stains, dark pigments, and necrotic bacterial matter, causing the affected area to turn a highly distinct brown, grey, or pitch-black color 11.
3. Heightened Dentinal Hypersensitivity
Once the incredibly hard, protective layer of enamel is successfully breached by bacteria, the significantly softer, underlying dentin is left entirely exposed to the oral environment. Because dentin contains thousands of microscopic fluid-filled tubules that connect directly to the inner nerve of the tooth, patients begin to experience sharp, fleeting jolts of intense pain whenever they consume hot beverages, freezing treats, or heavily sweetened foods 12.
4. Spontaneous or Lingering Pain
A persistent, heavy, and throbbing ache that originates entirely without any external provocation is a classic, undeniable clinical indicator that the bacterial infection has penetrated deeply enough to aggressively inflame the delicate, vascular pulp tissue inside the core of the tooth. This severe type of pain often radiates heavily through the jawbone, frequently disrupting normal sleep patterns and indicating irreversible nerve damage 13.
5. Discomfort Provoked by Mastication
Applying normal biting pressure to a severely decayed and structurally compromised tooth can instantly trigger acute, shooting pain. This localized agony happens because the mechanical force of the jaw closing compresses the inflamed, infected periapical tissues within the pulp chamber, or physically pushes the fractured, unsupported segments of the weakened tooth structure directly against the underlying sensitive nerves 14.
6. Development of a Localized Abscess
In highly advanced cases where the bacterial infection has completely eradicated the tooth’s internal nerve supply, massive colonies of bacteria spill out from the bottom tip of the root directly into the surrounding jawbone. This biological invasion generates a pressurized pocket of pus, medically termed an abscess, which typically manifests as a highly swollen, painful bump on the gums, severe facial swelling, and potentially life-threatening systemic fevers 15.
Tooth Decay (Cavities) Facts Table
| # Features | Details |
| Symptoms |
|
| Causes |
|
| Types of Tooth Decay (Cavities) |
|
| How does spread |
|
| Age Group |
|
| You might be at a higher risk for exposure of this disease if you: |
|
| How doctors diagnose |
|
| Other facts |
|
Natural Remedies for Tooth Decay (Cavities)
When facing the early stages of tooth decay, professional medical intervention is always the ultimate standard of care. However, an extensive body of modern scientific literature now strongly supports the adjunctive use of specific, naturally derived compounds to actively halt demineralization, suppress cariogenic bacterial growth, and physically rebuild damaged enamel.
1. Xylitol
Extracted primarily from the fibrous bark of birch wood and various other tough plant fibers, xylitol is a naturally occurring five-carbon sugar alcohol that serves the dietary world as a highly effective, low-calorie, non-nutritive sweetener. Mechanistically, the cariogenic bacteria responsible for decay, such as Streptococcus mutans, readily internalize xylitol through their complex, energy-consuming cellular pathways, critically misidentifying the molecule as a normal, metabolizable carbohydrate 16. However, because the primitive bacterial cellular machinery lacks the necessary enzymes to break down the resulting xylitol-5-phosphate compound, the organism derives absolutely no usable energy from the interaction, leading instead to a toxic accumulation of intracellular vacuoles and rapid, fatal cell membrane degradation 17. To survive, the bacteria must subsequently expend massive amounts of further energy to manually expel the useless molecule, trapping them in a completely futile, self-destructive metabolic loop that effectively starves the entire colony to death 18. Routine, daily consumption of this natural sugar drastically diminishes the overall pathogenic bacterial load in both saliva and resting dental plaque, substantially reduces the physical adhesiveness of the biofilm, and reliably neutralizes the acidic oral environment, thereby strongly facilitating the body’s natural remineralization cycle 19. Clinical trials continuously underscore that habituated, daily xylitol usage can successfully lower an individual’s overall lifetime caries risk by incredible margins, with the optimal preventative therapeutic thresholds resting firmly between 6 and 10 grams daily, divided strategically across multiple small exposures 20.
Note: Commonly consumed therapeutically in the form of sugar-free chewing gum, slowly dissolving lozenges, or specialized oral pediatric syrups, preferably utilized for several minutes immediately following all daily meals and snacks.
2. Nano-Hydroxyapatite (nHAp)
The burgeoning field of biomimetic nanotechnology has vastly popularized the integration of nano-hydroxyapatite, a brilliantly engineered synthetic compound designed to chemically, biologically, and structurally mirror the primary foundational mineral constituent of human teeth and bone 21. Natural, healthy dental enamel is essentially a tightly woven, incredibly dense matrix composed of 20 to 40-nanometer hydroxyapatite crystals. Because nHAp therapeutic particles are deliberately synthesized at this precise, identical nanoscale, they possess an extraordinary, unmatched capacity to directly and seamlessly integrate into the microscopic demineralized, porous regions of a decaying tooth 22. Unlike traditional chemical therapeutic agents that primarily promote a brittle, surface-level hardening, nHAp particles actually penetrate deeply into the collapsed subsurface architecture of an incipient carious lesion, actively replacing the lost calcium and phosphate ions from the inside out 23. Furthermore, this exceptional compound demonstrates profound clinical efficacy in managing agonizing dentinal hypersensitivity by physically acting as a plug, fully occluding the open, exposed dentinal tubules that lead directly to the tooth nerve 24. Extensive laboratory and live-patient studies routinely indicate that nHAp functions effectively as a completely non-toxic, highly biocompatible remineralizing agent, matching and occasionally greatly exceeding the reparative capabilities of conventional historical formulations without carrying any associated risks of systemic gastrointestinal toxicity upon accidental ingestion 25.
Note: Applied topically as the primary active therapeutic ingredient in highly specialized modern toothpastes or concentrated dental restorative serums, brushed firmly onto the teeth twice daily and ideally left entirely undisturbed without any immediate aqueous rinsing to fully maximize mineral uptake.

3. Theobromine (Cocoa Extract)
Derived entirely from the tough outer husk of the Theobroma cacao bean, theobromine is a highly bitter, water-soluble alkaloid compound that has surprisingly demonstrated remarkable, robust potential in the realm of preventative dentistry 26. Laboratory-grade microscopic analyses definitively reveal that theobromine interacts fundamentally with the foundational hydroxyapatite structure of the tooth, actively facilitating a massive increase in the physical size of the individual enamel crystallites 27. This resulting morphological enlargement renders the enamel surface significantly more robust, dramatically hardening the tooth and making it highly resistant to any subsequent bacterial acid dissolution 28. Beyond its undeniable structural benefits, theobromine exerts a measurable, potent antimicrobial activity by severely decreasing the physical deposition of Streptococcus mutans and Enterococcus faecalis biofilms, while simultaneously working to elevate the resting salivary pH of the mouth into a safer, alkaline state 29. Rigorous comparative clinical investigations involving various pediatric dental formulations have proven that dentifrices heavily featuring theobromine produce far greater zones of bacterial inhibition, and yield statistically significant, measurable enamel remineralization when stacked directly against several commercially dominant alternatives 30. Crucially, as a naturally occurring, deeply integrated dietary component, theobromine is completely safe to swallow, making it particularly advantageous and entirely risk-free for application in highly uncooperative young children and medically compromised individuals who cannot safely tolerate traditional chemical therapies 31.
Note: Commonly incorporated into high-end specialty non-fluoridated toothpaste formulations, daily therapeutic mouthwashes, or ingested functionally via high-percentage, incredibly low-sugar dark chocolate for localized, natural oral health benefits 32.
4. Licorice Root Extract
Rooted exceptionally deeply in the ancient practices of traditional holistic medicine, the natural extract of the licorice plant (Glycyrrhiza glabra) offers a remarkably potent arsenal of bioactive secondary metabolites, principally identifying glycyrrhizin, glabridin, licoricidin, and licorisoflavan A as its heavy hitters 33. These naturally occurring, complex phytochemicals exhibit profound, aggressive antimicrobial properties that specifically and effectively target the fundamental biological etiology of both rapid tooth decay and chronic periodontal disease. Scientific literature definitively affirms that licoricidin and licorisoflavan A function as highly potent inhibitors of Streptococcus mutans, successfully disrupting the microorganism’s core ability to synthesize the sticky, insoluble glucans that are absolutely necessary for initial plaque adhesion to the slick enamel pellicle 34. In addition to aggressively suppressing acidogenic caries-causing bacteria, the deeply soothing anti-inflammatory properties of glycyrrhetinic acid heavily modulate the host’s cellular immune response, vastly reducing the destructive release of pro-inflammatory cytokines such as interleukins, which significantly mitigates co-occurring, bleeding gingivitis 35. Furthermore, advanced confocal microscopy of damaged enamel blocks deliberately subjected to licorice extracts readily confirms enhanced visual remineralization and a completely arrested state of active demineralization, strongly suggesting a powerful dual-action mechanism of both bacterial suppression and crucial mineral preservation 36.
Note: Commonly utilized seamlessly as an active aqueous infusion in soothing herbal mouthwashes, incorporated heavily into natural organic toothpastes, or carefully chewed in its raw, dried root form to simultaneously stimulate heavy saliva production and deliver antibacterial agents directly to the gums 37.
5. Oil Pulling
Originating thousands of years ago from the ancient, holistic tenets of traditional Ayurvedic medicine, oil pulling is a highly demanding adjunctive mechanical and biological oral hygiene practice that involves the extended, vigorous swishing of high-quality edible oils predominantly organic coconut, sesame, or extra-virgin olive oil deeply within the oral cavity 38. The constant physical agitation of the thick, viscous lipid substance creates an immense, fluid shear force that actively pulls rotting food debris, dead cellular matter, and loosely adhered bacterial plaque directly from the tight interproximal spaces of the teeth 39. Biologically, the prolonged swirling process induces a chemical reaction known as saponification, wherein the naturally alkaline environment of the human saliva forcefully interacts with the complex triglycerides found in the oil, essentially creating a natural, microscopic soap that permanently compromises the lipid-based cell membranes of various harmful microorganisms 40. Strict clinical assessments readily verify that a highly consistent, daily regimen of oil pulling can reliably reduce the total oral microbial count by up to 20%, specifically curtailing the rampant proliferation of Streptococcus mutans, Lactobacilli, and the fungal pathogen Candida albicans 41. Independent studies comparing high-grade olive oil to standard chemical chlorhexidine medical rinses noted highly comparable, excellent reductions in overall caries activity and bleeding gingival inflammation scores, confirming its absolute validity as a safe natural therapeutic adjunct 42.
Note: Practiced strictly by swishing exactly one tablespoon of organic oil vigorously around the mouth and forcefully through the teeth for 10 to 20 uninterrupted minutes, usually on an empty stomach in the early morning, followed by spitting the emulsified, toxic liquid entirely into a waste receptacle (never swallowed) and completing a normal brushing routine.
6. Green Tea Extract
The raw, completely unoxidized leaves of the Camellia sinensis plant, universally brewed and consumed as green tea, yield an incredibly rich aqueous infusion heavily saturated with highly active antioxidant polyphenols, most notably the incredibly potent catechin epigallocatechin gallate (EGCG) 43. Medical research confirms that EGCG demonstrates exceptional, rapid bactericidal properties by irreversibly binding directly to, and structurally damaging, the vital cytoplasmic membranes of acid-producing oral bacteria, thereby entirely preventing their colonization and eventual thick biofilm maturation 44. Additionally, the green tea plant naturally bioaccumulates high trace amounts of organic fluoride directly from the deep soil, which works perfectly synergistically with the circulating organic catechins to confer highly heightened, measurable acid resistance to the human enamel structure 45. Regular, daily exposure to strong green tea extract directly and heavily inhibits bacterial salivary amylase activity, effectively stalling the rapid breakdown of dietary starches into dangerous fermentable sugars right inside the warm oral cavity before the bacteria can ever reach them 46. The powerful dual action of heavily minimizing the metabolic food substrate available for bacteria, while simultaneously directly destroying their microscopic cellular integrity, makes green tea extract an absolutely formidable natural intervention against both the initiation and rapid progression of carious lesions 47.
Note: Commonly consumed multiple times daily as a freshly brewed, entirely unsweetened hot beverage, or utilized topically as a highly standardized botanical extract incorporated directly into therapeutic daily mouthrinses and natural dentifrices.
7. Turmeric and Ginger
While historically celebrated primarily in the culinary and medicinal healing traditions of India and China for their potent, unmatched systemic anti-inflammatory effects, both turmeric (containing curcumin) and raw ginger offer highly unique, localized, and proven benefits for direct dental health preservation 4. The deliberate, synergistic topical application of these finely ground rhizome powders aggressively addresses the chronic, painful inflammatory responses of the soft gingival tissues that almost always accompany rampant, unchecked tooth decay. In the highly specific context of dental hard tissue preservation, contemporary in vitro studies have decisively demonstrated that pure extracts of both ginger and turmeric facilitate a truly remarkable, visible remineralizing effect on early, incipient carious lesions 48. These powerful botanicals exert massive antibacterial and antioxidant qualities that rapidly neutralize the destructive oxidative stress and highly acidic environment artificially created by cariogenic pathogens. Although the precise, molecular ionic mechanisms remain under active microscopic investigation, their undeniable ability to chemically stabilize the oral microenvironment strongly supports the natural, unhindered precipitation of vital salivary minerals back into the damaged, porous enamel matrix.
Note: Commonly formulated carefully into homemade or commercial herbal tooth powders, blended thickly with a carrier oil to form a localized healing poultice for painful affected teeth, or utilized as an incredibly strong aqueous botanical mouth rinse.
8. Eggshell Powder
Chicken eggshells represent an incredibly highly concentrated, completely biologically derived natural source of pure calcium carbonate, alongside crucial trace amounts of vital structural minerals such as magnesium and phosphorus 49. Due to its highly specific chemical composition, which incredibly closely mimics the inorganic foundational matrix of human bone and developing teeth, eggshell powder has been heavily and successfully researched in advanced bone graft regeneration and, more recently, in active dental remineralization protocols. When processed correctly and carefully into a fine, non-abrasive micro-particulate powder, the massive bioavailability of the calcium carbonate allows it to readily and easily interact with the natural oral fluids. Preliminary in vitro research evaluating the direct application of pure chicken eggshell powder (CESP) on damaged primary teeth notes its incredible effectiveness in fully remineralizing early-stage, non-cavitated enamel lesions by physically flooding the local oral environment with the absolute essential building blocks required to completely rebuild the complex hydroxyapatite crystalline lattice from the ground up.
Note: Commonly heavily sterilized via boiling, pulverized meticulously into a micro-fine dust, and integrated fully into homemade remineralizing toothpastes, or taken internally as a powerful daily dietary supplement to fortify deep systemic calcium reserves.
Is there any exercise or physical activities for Tooth Decay (Cavities)
Beyond topical applications, specific neuromuscular and physical exercises can significantly elevate the mouth’s natural defense mechanisms by manipulating the salivary glands and surrounding musculature.
1. Tongue Rotation Exercises
A highly comprehensive, deliberate neuromuscular exercise targeting the entire stomatognathic system, tongue rotation physically engages a vast network of intraoral and thick cervical muscles, including the powerful genioglossus, hyoglossus, and masseter 50. This deliberate, forced muscular activation places immense physical pressure directly on the minor and major salivary glands while simultaneously strongly stimulating the parasympathetic vagus nerve. The sudden activation of this deep neural pathway not only triggers a massive, sudden influx of both stimulated and unstimulated whole saliva, but also actively depresses the secretion of harmful salivary stress hormones like amylase. Clinical metrics clearly show that correctly performing this simple exercise increases total saliva volume by up to 25% within mere minutes, creating a massive alkaline wash that instantly neutralizes the localized acidic environments responsible for rampant dental decay.
Note: Performed seamlessly by keeping the lips firmly sealed shut and pressing the sharp apex of the tongue hard against the outer surface of the gums, slowly tracing a wide, continuous circle inside the mouth. The tongue is rotated 20 times in a slow clockwise direction, followed immediately by 20 firm counterclockwise rotations.
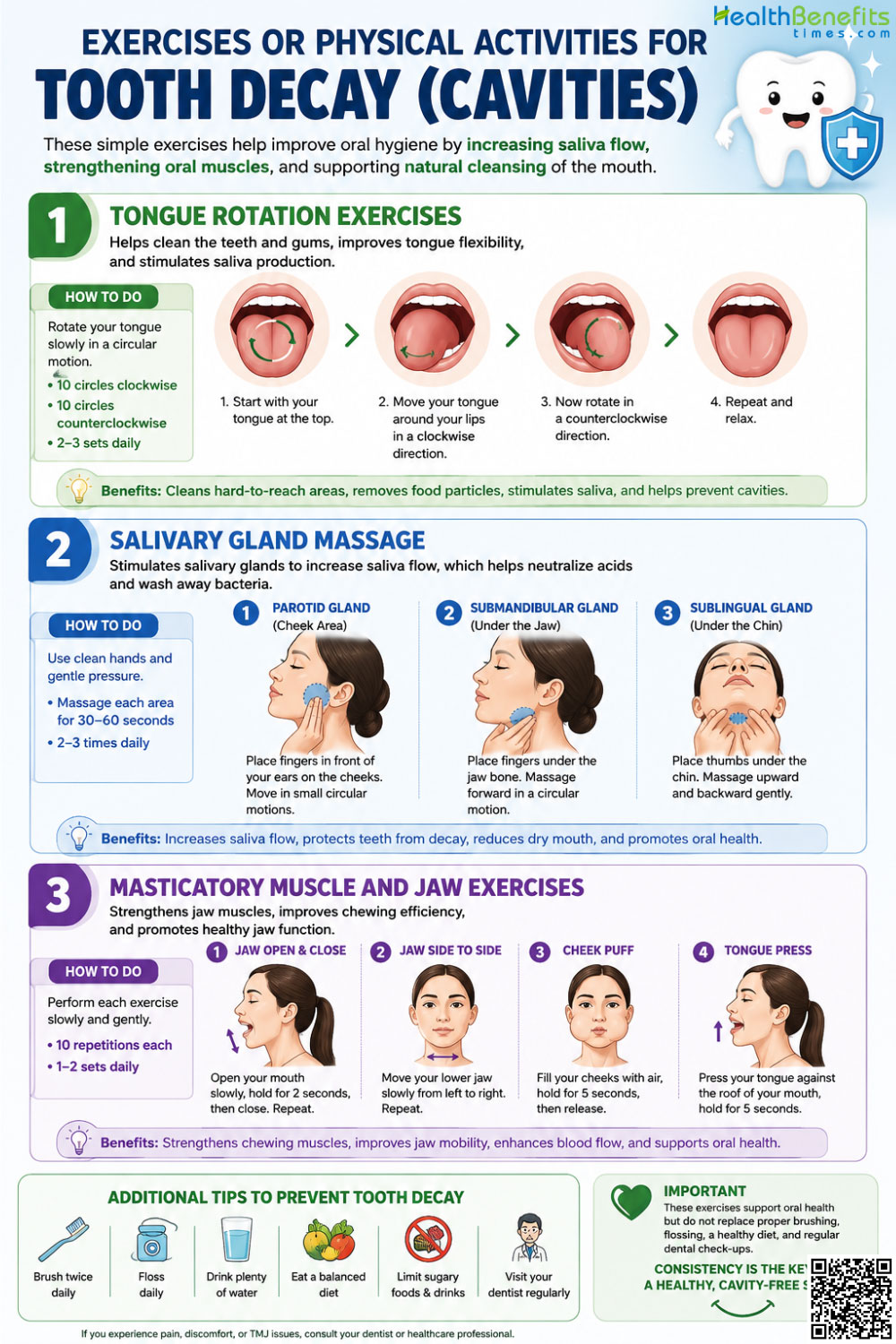
2. Salivary Gland Massage
The direct mechanical stimulation of the major salivary glands namely the large parotid, submandibular, and sublingual glands serves as a highly effective, immediate physical intervention to forcefully increase salivary flow, which remains the human body’s absolute primary biological defense against acid demineralization 51. Saliva naturally and constantly flushes acidic byproducts, delivers heavy remineralizing ions, and contains incredibly protective immune immunoglobulins. Manual, deep-tissue massage forcefully expels stagnant, pooled saliva from the deep glandular acini straight through the specific excretory ducts and directly into the oral cavity, providing immediate, profound relief for patients suffering from severe xerostomia (dry mouth) 52. To execute this correctly, firm pressure is applied externally to the face and neck. For the large parotid gland, two fingers are placed directly in front of the earlobe, sliding firmly forward over the cheek with gentle, sustained pressure to encourage heavy flow through Stensen’s duct 53. For the lower submandibular and sublingual glands, fingers are positioned deeply beneath the inferior bony border of the mandible (jawbone), sliding anteriorly toward the front chin to push thick fluid rapidly through Wharton’s duct 54.
Note: Performed gently by applying firm, warm, forward-sliding pressure continuously over the specific glands for 1 to 2 unbroken minutes per region, ideally 2 to 3 times daily, to consistently and permanently elevate the resting salivary flow rate over time.
3. Masticatory Muscle and Jaw Exercises
The fundamental biological act of mastication operates universally as the absolute primary physiological trigger for heavy salivary secretion 55. Engaging the thick jaw muscles through deliberate empty chewing, forceful clenching exercises, or utilizing specialized intraoral vibration devices dramatically facilitates heavy local blood flow and fast metabolic turnover in the entire orofacial region. A highly structured, repetitive routine of empty chewing followed instantly by deep, forceful inhalation, breath-holding, and consecutive empty swallowing can consistently and permanently train the nervous system to heavily elevate baseline salivary output 56. Because the heavy mechanical loading of the thousands of periodontal ligaments directly communicates with the lower brain stem to trigger immediate saliva release, these specific jaw exercises are absolutely invaluable for elderly populations or chronically ill individuals suffering from severe, medication-induced hyposalivation.
Note: Practiced easily by mimicking a highly forceful, incredibly exaggerated chewing motion without the actual presence of any food for several continuous minutes, alternating rapidly with forceful dry swallowing, to artificially trigger the body’s natural, heavy digestive lubrication response.
Activities to Avoid When You suffer from Tooth Decay (Cavities)
1. Brushing Immediately After Vomiting or Acid Reflux
Following a violent emesis event or a severe acid reflux episode, your tooth enamel is highly chemically softened by stomach acid. Vigorously brushing your teeth immediately after this acidic exposure mechanically and permanently strips away this decalcified, incredibly vulnerable layer of your tooth 57. You must absolutely wait a minimum of 30 minutes to allow your natural saliva to neutralize the acid and harden the surface before attempting any mechanical brushing.

2. Mouth Breathing
Chronic respiration directly through your mouth, particularly during the long hours of your sleep, entirely halts the protective, washing mechanisms of your saliva. This dangerous activity drastically lowers your intraoral pH, completely dehydrates your gingival tissues, and dramatically elevates your risk of severe, painful anterior dental caries.
3. Sleeping in a Supine Position
Lying completely flat immediately after consuming a heavy meal allows highly corrosive gastric acids to flow freely and easily into your esophagus and mouth. You are strongly advised to permanently elevate the head of your bed or sleep specifically in the left lateral decubitus position to intelligently harness gravity against upward acid regurgitation 58.
4. Sipping Sugary Drinks Slowly Over Time
Prolonging the consumption of a sweetened beverage over several hours ensures that your mouth remains in a state of constant, unbroken acidic attack. You should consume beverages quickly to allow your saliva the necessary time to recover its baseline pH 8.
Myths and Misconceptions
| Myth | Reality |
| Brushing teeth immediately after vomiting or an acid reflux attack protects them from stomach acid. | Vigorously brushing directly after an acidic event severely and permanently damages the teeth. The acid heavily softens the enamel, and the abrasive action of a toothbrush physically strips this weakened layer away forever. Rinsing gently with water and waiting at least 30 minutes is absolutely required. |
| Cavities occurring in primary baby teeth do not matter because they will eventually fall out anyway. | Rampant Early Childhood Caries (ECC) can rapidly lead to severe agony, life-threatening systemic abscesses, malnourishment, and delayed speech. Furthermore, the premature loss of primary teeth permanently compromises the spatial alignment of the developing permanent adult dentition. |
| Chemical fluoride is the absolute only substance capable of remineralizing damaged tooth enamel. | While undeniably highly effective, fluoride is not biologically unique in this capacity. Synthesized nano-hydroxyapatite, natural xylitol, theobromine (cocoa extract), and various botanical polyphenols have been scientifically, rigorously proven to drive heavy remineralization and entirely halt decay progression. |
| A chronic dry mouth is just a minor, temporary annoyance and is unrelated to actual serious dental diseases. | Saliva is the oral cavity’s absolute primary, critical biological defense mechanism. A chronic, daily lack of saliva (xerostomia) entirely removes the mouth’s ability to buffer acids and supply repairing minerals, causing a truly catastrophic, rapid acceleration in the rate of total tooth decay. |
| Consuming a massive amount of natural xylitol will quickly and safely eliminate all oral bacteria in one day. | Exceeding the standard, recommended daily dosage of xylitol does not confer any additional, magical dental benefits; instead, high dosages (exceeding 40-45 grams daily) act as a severe osmotic laxative in the human gut, resulting in extreme gastrointestinal distress, cramping, and severe diarrhea. |
Special Considerations
1. Children
The pediatric population exhibits profound, unmatched biological vulnerability to aggressive tooth decay, primarily due to the specific anatomical and developmental characteristics of primary (deciduous) dentition. The protective enamel on baby teeth is biologically formed over a highly accelerated 24-month period, resulting in a fragile outer layer that is exactly half the physical thickness of adult permanent teeth and possesses a vastly less organized, highly porous crystalline microstructure 61. Consequently, cariogenic acids can easily demineralize deciduous enamel at a significantly faster, more aggressive rate 62. This innate structural fragility underscores the devastating phenomenon of Early Childhood Caries (ECC), which frequently completely destroys the maxillary anterior teeth of vulnerable infants who are repeatedly exposed to sugary liquids via prolonged baby bottles or extended, unmonitored breastfeeding at night 63. Furthermore, common behavioral adaptations such as chronic mouth breathing or heavy pacifier dependency dramatically alter the salivary environment, massively exacerbating the prevalence of carious lesions in preschoolers 64. Proactive, daily measures, including consistent topical remineralization therapies and extremely strict dietary limits on fermentable carbohydrates, are absolutely mandatory to protect this highly vulnerable demographic 65.
2. Pregnancy
The biological process of pregnancy initiates a highly complex, sweeping cascade of physiological, immunological, and massive hormonal changes that drastically compromise the normally stable oral environment 66. Elevated, surging levels of circulating steroid hormones aggressively alter the vascular permeability of the delicate gingival tissues, frequently precipitating severe pregnancy gingivitis and highly destructive periodontitis 67. From a strictly cariogenic perspective, expectant mothers frequently experience intense shifts in daily dietary cravings heavily skewed toward high-carbohydrate foods, coupled seamlessly with a measurable, dangerous reduction in salivary pH and total buffering capacity during the final, heaviest trimesters 68. Furthermore, the onset of hyperemesis gravidarum (severe, repetitive morning sickness) introduces incredibly potent gastric acids directly into the mouth on a daily basis, driving rampant, unchecked enamel erosion 69. Additionally, the vertical, direct transmission of Streptococcus mutans from a heavily infected mother to her newborn infant is a primary vector for severe childhood decay. Scientific, clinical protocols strongly suggest that if an expectant mother routinely consumes therapeutic, daily doses of xylitol during her pregnancy, she can significantly and permanently suppress her own bacterial load, thereby delaying or entirely preventing the microbial colonization of her newborn’s pristine oral cavity 70.
3. Chronic Conditions
Systemic, lifelong chronic diseases inherently and permanently disrupt the delicate biological homeostasis required for maintaining optimal oral health. Diabetes mellitus, encompassing both Type 1 and Type 2, presents a unique, devastating dual-threat mechanism to the human mouth. Severe systemic hyperglycemia results directly in highly elevated glucose concentrations within the salivary fluid itself, continuously bathing the teeth in a rich, fermentable substrate that relentlessly fuels bacterial acid production day and night 71. Simultaneously, the onset of diabetic neuropathy and severe vascular changes frequently induce severe, chronic xerostomia (hyposalivation), entirely neutralizing the body’s mechanical washing capability and permanently preventing the necessary delivery of reparative calcium ions to the starving enamel 7. The combination of high sugar in the saliva and low saliva volume creates a perfect storm for rapid tooth loss 72. Similarly, individuals afflicted with severe Gastroesophageal Reflux Disease (GERD) or complex psychiatric eating disorders (such as bulimia nervosa) face relentless, daily intrinsic acid challenges 73. Gastric acid registers at a pH incredibly low enough to instantly dissolve the protective acquired pellicle immediately upon contact, leading rapidly to irreversible, catastrophic erosive tooth wear, particularly heavily concentrated on the palatal surfaces of the maxillary incisors 74.
4. Elderly
The aging geriatric demographic faces a highly unique, structural architectural shift in disease presentation, transitioning rapidly from standard coronal (crown) decay to highly aggressive, rampant root caries 75. As individuals advance significantly in age, cumulative lifetime periodontal disease and heavy mechanical wear cause the gingival soft tissues to recede permanently, exposing the underlying, softer cementum and dentin of the vulnerable tooth roots 76. Because root surfaces entirely lack the protective, highly mineralized enamel cap found on the crown, they are rendered exceptionally, uniquely susceptible to incredibly rapid decay at much higher, normally safe pH levels 77. The elderly are also highly prone to massive polypharmacy the daily, routine consumption of multiple, overlapping prescription medications which almost always frequently yields severe drug-induced xerostomia 78. This profound, chronic lack of saliva, combined seamlessly with natural age-related decreases in fine manual dexterity necessary for proper brushing, and a dietary reliance on softer, simpler carbohydrates due to missing teeth or ill-fitting dentures, creates a notoriously high-risk matrix for runaway, devastating dental destruction in older populations 79.
Precaution before use of natural remedies when you have Tooth Decay (Cavities)
While holistic and botanical interventions offer substantial, scientifically backed therapeutic benefits, you must approach them with rigorous caution, precise dosing, and a thorough understanding of their physical and physiological limits.
- Xylitol Gastrointestinal Distress: You must be aware that xylitol operates as a powerful osmotic agent within your human digestive tract. While a daily therapeutic dose of 6 to 10 grams is entirely safe and optimal for your dental care, excessive ingestion (exceeding 45 grams) will rapidly draw massive amounts of water into your intestines, triggering severe abdominal cramping, loose stools, and violent osmotic diarrhea.
- Toxicity in Oil Pulling Emulsions: The fundamental mechanism of your oil pulling routine relies entirely on the lipid extraction of oral bacteria. Consequently, the resulting milky fluid you generate after 15 minutes of swishing is heavily saturated with live microbes, necrotic tissue, and toxins. You must expectorate this emulsified mixture entirely into a waste bin and never swallow it, as systemic ingestion can easily provoke gastrointestinal illness.
- Aspiration Risks for Children: You must strictly avoid utilizing the oil pulling technique on any children under the age of five. The prolonged swishing of a thick lipid carries an exceptionally high risk of accidental choking or aspiration of the bacteria-laden oil directly into their developing lungs.
- Severe Abrasiveness of Powders: Utilizing homemade dental pastes formulated with your own coarse, unrefined eggshell powder or raw botanical spices (like turmeric) can be excessively, dangerously abrasive. If you do not micro-pulverize these items, the jagged particulate matter will physically scour your fragile enamel and severely exacerbate your gingival recession.
- Allergic Reactions to Botanicals: Concentrated botanical extracts, including your licorice root and green tea tinctures, contain incredibly potent phytochemicals that may provoke localized contact dermatitis in your mouth or interact poorly with your systemic medications. For example, high sustained consumption of glycyrrhizin from licorice root can dangerously influence your blood potassium levels and spike your blood pressure.
When to see a Doctor
The aggressive progression of dental caries is strictly unidirectional without professional intervention; at critical junctures, your natural remedies are entirely insufficient, and immediate professional medical or dental care is absolutely imperative to prevent severe, life-threatening systemic complications.
- Spontaneous or Nocturnal Pain: If your tooth exhibits a severe, unprovoked throbbing pain that actively disrupts your sleep or does not abate with the removal of hot or cold stimuli, the bacterial infection has likely successfully breached the enamel and dentin, heavily infiltrating your deep vascular pulp chamber.
- Visible Swelling or Abscess Formation: The sudden appearance of a purulent, pimple-like lesion on your gums, accompanied by heavy facial swelling, localized heat, or an associated high fever, signifies a severe bacterial abscess. You must seek immediate care, as this localized infection can rapidly track into the deep fascial spaces of your head and neck, obstructing your airways or causing life-threatening sepsis.
- Severe Dentinal Hypersensitivity: A sudden, incredibly sharp, and lingering physical response to thermal changes (hot/cold) or osmotic pressure (sugary foods) strongly indicates advanced structural loss that exposes your underlying nervous tissue, requiring professional sealants, fillings, or restorative intervention to fix.
- Signs of Silent Acid Reflux: The development of inexplicable, widespread enamel erosion, particularly heavily concentrated on the inner (palatal) surfaces of your upper teeth, often accompanied by a persistent sour taste, warrants your immediate referral to a medical gastroenterologist to diagnose and manage underlying, highly destructive silent GERD.
- Chronic Salivary Gland Pain: Persistent swelling, deep pain, or fever localized directly over your cheek or jaw area that lasts for three or more consecutive days suggests a severe salivary gland infection (sialadenitis) or a physical glandular blockage, necessitating your immediate professional diagnostic imaging and potential, heavy antibiotic therapy.
Comments
comments