
Trapped water in the ear refers to the accumulation and retention of moisture within the external auditory canal, typically occurring after swimming, bathing, or heavy sweating. Because the ear canal is narrow, dark, and naturally curved, water can easily become lodged behind anatomical bends or pre-existing earwax blockages. While not a medical diagnosis itself, trapped fluid is a significant clinical risk factor for infections. Prolonged moisture macerates the delicate skin lining the canal and neutralizes its naturally protective, acidic cerumen (earwax) barrier. This compromised environment actively promotes the rapid multiplication of opportunistic bacteria and fungi, frequently leading to acute otitis externa, widely known as swimmer’s ear 1. The primary symptoms include a distinct sensation of fullness, muffled hearing, a tickling or “sloshing” feeling, and mild discomfort. If the water does not drain naturally, safe drying techniques are necessary to prevent painful structural inflammation and potential temporary hearing impairment 2, 3, 4, 5.
The Anatomy and Physiology of the Ear Canal
Delving into the structural layout of the human auditory system reveals precisely why moisture occasionally refuses to drain naturally. The external auditory canal is an intricately shaped tunnel measuring approximately 2.5 centimeters in length, serving as the primary conduit from the visible outer ear to the sensitive tympanic membrane 6. Functionally, it collects ambient sound waves and funnels them efficiently toward the middle ear space, but its internal architecture is remarkably complex. The lateral, outward-facing half of this canal consists of elastic cartilage and features a relatively thick dermal layer equipped with hair follicles, sebaceous glands, and specialized apocrine sweat glands 7. Conversely, the medial half tunnels directly through the dense temporal bone of the skull. Skin lining this deeper, osseous section is exceptionally thin, anchored directly to the underlying periosteum, and completely lacks any protective subcutaneous fat layer, rendering it highly susceptible to physical trauma and temperature fluctuations 8.
Observing where these two distinct anatomical regions intersect, one finds a natural structural bottleneck clinically recognized as the isthmus. This physiological narrowing is positioned just a few millimeters outward from the eardrum and serves a critical protective function by preventing foreign objects and insects from easily striking the delicate tympanic membrane 9. However, this identical choke point creates a physical harbor where liquids can easily become marooned. When water successfully bypasses this narrow junction, the surface tension of the liquid, interacting with the extremely small diameter of the space, generates strong capillary action. Consequently, the fluid forms a stubborn meniscus that bridges the walls of the bony canal, securely locking the moisture in place with a force that readily overcomes standard gravity.
Beyond the physical topography, the biochemical environment of the canal is equally instrumental in fluid management. Specialized glands situated in the outer cartilaginous zone continuously synthesize cerumen, universally recognized as earwax, which represents a sophisticated biological matrix of shed epithelial cells, long-chain fatty acids, squalene, and distinct alcohols 10. This specific chemical composition endows healthy earwax with robust hydrophobic, or water-repelling, characteristics. Under normal circumstances, ambient water simply beads up against this waxy barrier and rolls harmlessly out of the ear. Furthermore, a healthy cerumen layer maintains a distinctly acidic environment—typically registering a pH between 4.0 and 5.0—which acts as a hostile barrier to opportunistic pathogens.
How to Know There is Trapped Water in the Ear
Recognizing the specific clinical indicators of fluid retention in the external ear canal is the initial step toward achieving effective relief. Because the auditory canal is a highly sensitive organ richly innervated by multiple cranial nerves, even a minuscule droplet of liquid resting against the eardrum triggers pronounced sensory feedback.
- Aural Fullness: Patients frequently report a distinct, heavy sensation of pressure or complete blockage on one side of the head, creating a feeling akin to the ear being tightly stuffed with cotton 4.
- Muffled or Diminished Hearing: Sound waves struggle to propagate efficiently through a liquid medium compared to air, which induces a temporary conductive hearing loss where voices and environmental noises appear distant, hollow, or unusually muffled 2.
- Crackling or Sloshing Sounds: Shifting the jaw, swallowing, or simply tilting the head often produces highly audible bubbling, shifting, or crackling noises as the fluid meniscus continuously breaks and reforms against the tympanic membrane.
- Temperature Sensitivity: Because the epithelial lining of the inner bony canal is remarkably thin, trapped water that cools below the body’s core temperature can trigger a sudden, highly localized sensation of coldness deep within the skull.
- Mild Tickling or Pruritus: As the liquid slowly shifts position or begins the process of evaporation, it can stimulate the fine hairs and superficial nerve endings in the outer canal, inciting a distracting tickle or a profound urge to scratch the internal tissues 3.
- Otalgia (Ear Pain): While isolated fluid retention is traditionally painless, if the moisture persists long enough to cause cerumen to swell aggressively against the canal walls, or if the skin undergoes maceration, a dull ache or sharp pain may gradually emerge 11.
- Clear or Watery Drainage: Intermittently, assuming specific postures—such as lying flat to sleep—will permit a small volume of warm, clear fluid to unexpectedly trickle onto the outer ear or pillow as gravitational forces finally conquer the capillary surface tension.
The Pathophysiology of Moisture Retention
Investigating the underlying reasons why water becomes trapped necessitates a closer evaluation of the environmental and biological variables influencing the ear. For the vast majority of individuals, fluid introduced during a rapid shower or a vigorous lap in a swimming pool exits the canal almost instantaneously. The intertragic notch, a subtle anatomical groove positioned at the inferior aspect of the visible outer ear, naturally functions as a drainage spout for splashing water, actively routing droplets away from the canal’s entrance 12. Whenever this inherent drainage system fails, the root cause usually stems from a specific disruption in the ear’s delicate homeostatic equilibrium.
One major physiological contributor to fluid trapping involves the disruption of the skin’s natural “conveyor belt” clearance mechanism. Epithelial cells lining the tympanic membrane and the adjacent bony canal exhibit a fascinating biological trait known as directional desquamation 4. Unlike dermal cells on the rest of the human body, which flake off vertically upon apoptosis, the cells in the auditory canal migrate horizontally outward at a rate mirroring fingernail growth. This continuous, glacial outward movement naturally carries microscopic debris, old cerumen, and minor amounts of moisture out toward the ear’s exit. When an individual habitually utilizes cotton swabs or consistently wears tight-fitting earplugs, they physically disrupt this migration, shoving debris backward and creating an artificial dam.
Another significant structural factor is the presence of benign osteomas or external auditory exostoses, frequently referred to in coastal communities as “surfer’s ear.” People who spend extensive periods immersed in cold water and frigid winds such as avid surfers, deep-sea divers, and kayakers regularly develop these irreversible bone spurs inside the canal as a protective biological reaction to the chilling thermal exposure 13. These stony growths construct an uneven, mountainous landscape within the normally smooth tubular passage. Water easily washes over these prominent bony ridges but becomes inextricably trapped in the deep valleys between them, leading to chronic water pooling and an exponentially higher incidence of outer ear infections.
Furthermore, the chemical transformation that unfolds when water stagnates in the ear is clinically profound. Tap water and chlorinated pool water generally present as neutral to slightly alkaline solutions. When this fluid rests inside the normally acidic ear canal, it instantly elevates the localized pH, effectively neutralizing the ear’s primary chemical defense system. Simultaneously, constant moisture forces the superficial layers of the skin to aggressively absorb water and swell a degenerative process termed maceration 5. Macerated tissue loses its structural integrity, dismantling the physical barrier that actively prevents ambient environmental bacteria from invading the deeper dermal layers.
| Factor Influencing Water Trapping | Primary Mechanism of Action | Clinical Consequence |
| Isthmus Constriction | Creates a narrow anatomical choke point that exponentially increases capillary surface tension. | Prevents the natural gravity-assisted drainage of introduced fluids. |
| Cerumen Impaction | Dry, hygroscopic wax absorbs incoming water, swelling significantly to block the entire canal. | Induces a feeling of aural fullness, muffled hearing, and physical obstruction. |
| Epithelial Migration Failure | Halts the natural outward cellular transport of microscopic debris and desquamated skin. | Forms structural dams deep within the canal that effortlessly trap ambient moisture. |
| Auditory Exostoses | Chronic cold exposure triggers bony growths that create irregular, deep valleys in the canal floor. | Leads to chronic, recurrent pooling of water immediately after any swimming activity. |
How to Remove Trapped Water from Your Ear
Addressing a blocked ear canal requires a tactical approach aimed at safely breaking the surface tension of the fluid or encouraging rapid evaporation without inflicting trauma on the delicate internal tissues. You can effectively clear your ear by relying on fundamental principles of gravity, fluid dynamics, and basic chemistry through the following proven techniques.
1. Gravity and Head Positioning
Harnessing the natural pull of gravity is frequently the most straightforward and effective method for overcoming the fluid’s stubborn surface tension. You should stand or sit in an upright posture and sharply tilt your head so that the affected ear points directly downward toward your shoulder. To amplify the gravitational pull, you can perform a gentle hopping motion on one foot or vigorously shake your head from side to side 14. The sudden introduction of kinetic energy, paired with downward force, is routinely sufficient to dislodge the water droplet from the narrow isthmus. If you favor a more passive strategy, lying down on your side with the affected ear resting firmly on a soft towel for several minutes allows the water to slowly seep out unimpeded.
Note: This positional technique is commonly used as an immediate, non-invasive physical remedy to safely drain excess liquid without necessitating any internal mechanical intervention.
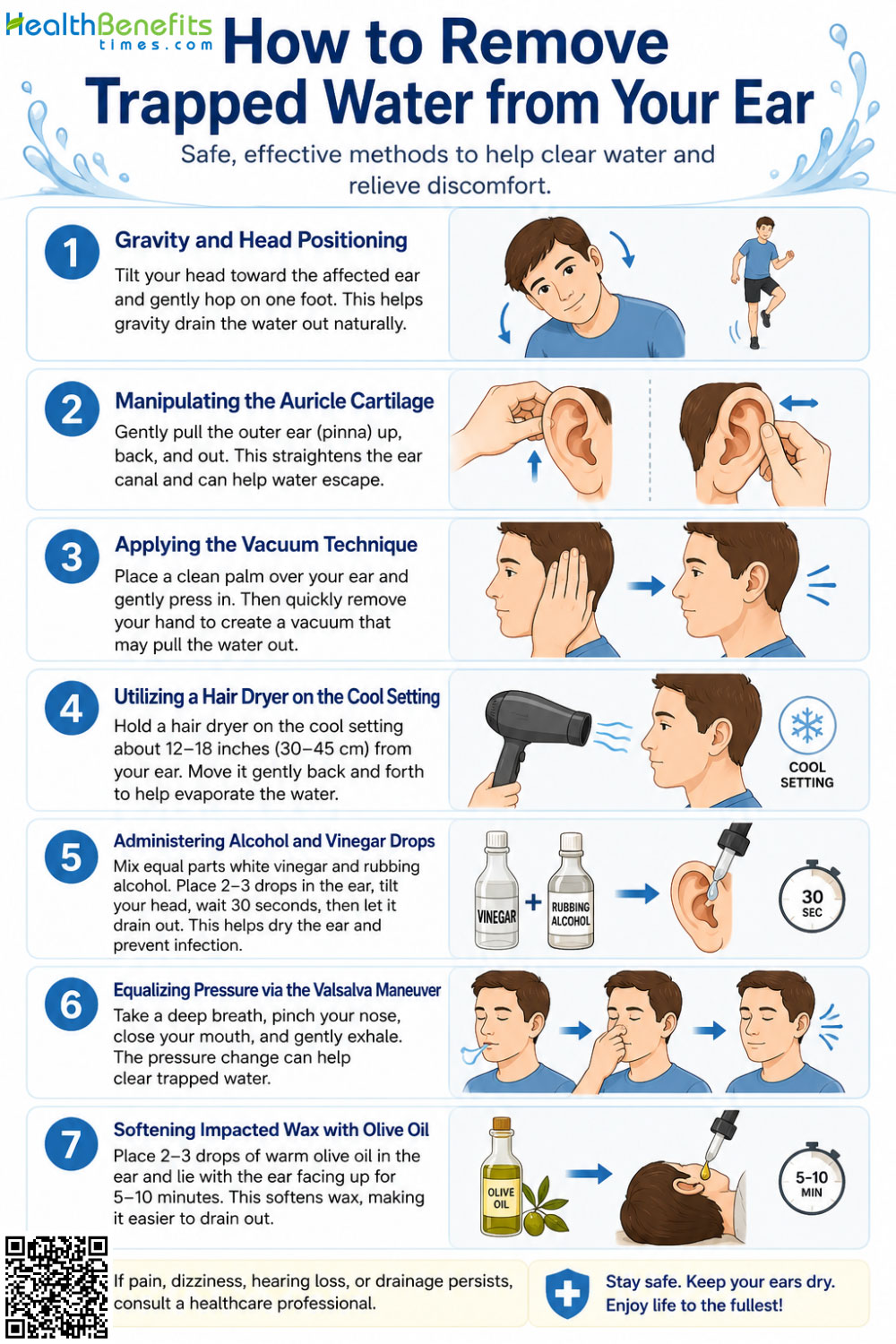
2. Manipulating the Auricle Cartilage
Because the human ear canal is not a perfectly straight tube it possesses a slight “S” shaped curvature water easily pools in the lower anatomical bends. You can manually straighten this convoluted pathway to provide the trapped water with a clear, unobstructed exit route. Reach up with your hand, grasp the outer cartilage of your ear (the pinna) or your lower earlobe, and gently pull it backward and downward. While securely holding the ear in this stretched position, tilt your head toward the floor. Straightening the natural curve temporarily eliminates the physical anatomical shelves where water rests, allowing it to flow out smoothly.
Note: This manipulation is commonly applied to rapidly clear the ear canal immediately after exiting a swimming pool by modifying the surrounding cartilaginous structure.
3. Applying the Vacuum Technique
Utilizing the basic principles of air pressure allows you to physically draw the recalcitrant water outward. Tilt your head sideways and place the flat palm of your hand tightly against your ear, ensuring that you create a complete, airtight seal over the entire outer auricle. Rapidly push your hand inward and cup it outward in a gentle, rhythmic pumping motion, taking care not to strike your head aggressively. This repetitive action compresses the air trapped inside the canal and subsequently generates a mild vacuum upon release. The fluctuating pressure gradient acts much like a miniature plunger, pulling the stubborn fluid droplet away from the eardrum and out toward the external opening.
Note: This pneumatic technique is effectively used to break the liquid meniscus deep within the ear by leveraging safe, controlled air pressure fluctuations.
4. Utilizing a Hair Dryer on the Cool Setting
If physical manipulation fails to clear the obstruction, thermal evaporation serves as a highly effective and safe alternative. You can utilize a standard handheld hair dryer to gently blow moving air into the ear canal. It is absolutely imperative that you set the device to its lowest possible fan speed and its coolest, lowest heat setting to entirely prevent thermal injury to the highly sensitive tympanic membrane 15. Hold the dryer several inches away from your head—never placing the nozzle directly against the ear opening and move it in a slow, continuous back-and-forth sweeping motion. The steady current of dry air dramatically accelerates the natural evaporation of the trapped moisture, gradually clearing the blockage without requiring any direct physical contact.
Note: This evaporative method is commonly used as a safe drying application to prevent moisture-related infections in individuals who are highly prone to chronic swimmer’s ear.
5. Administering Alcohol and Vinegar Drops
For fluid that stubbornly refuses to evaporate, creating a homemade chemical drying agent can yield incredibly rapid results. You can easily mix a solution consisting of equal parts standard rubbing alcohol (isopropyl alcohol) and white vinegar (acetic acid) 16. Using a clean, sterile dropper, instill three to four drops of this specific mixture directly into the affected ear, allow it to sit for approximately 30 seconds, and then tilt your head sideways to let it drain completely. The rubbing alcohol fundamentally lowers the surface tension of the trapped water, enabling it to mix and evaporate rapidly, while the white vinegar effectively restores the ear canal’s natural acidic pH, which actively eradicates aggressive bacteria and fungi. You must strictly avoid this method if you have a known perforated eardrum or surgically implanted ear tubes.
Note: This chemical remedy is commonly applied to achieve both the rapid desiccation of trapped fluids and robust broad-spectrum antimicrobial prophylaxis against otitis externa.
6. Equalizing Pressure via the Valsalva Maneuver
Occasionally, the distracting sensation of trapped water is actually a manifestation of unequal pressure within the Eustachian tube rather than actual fluid resting in the outer canal. You can attempt to manually equalize this internal pressure by performing the Valsalva maneuver. To execute this correctly, pinch your nostrils tightly closed, shut your mouth completely, and gently blow air out through your nose as if you are trying to inflate a stiff balloon. You will likely feel a distinct popping or clicking sensation in your ears as the internal pressure normalizes. Alternatively, you can widely yawn or mimic an exaggerated chewing motion. The temporomandibular joint is situated directly adjacent to the ear canal and Eustachian tube; moving the jaw forcefully massages the surrounding tissues and helps dislodge both trapped air and fluid.
Note: This physiological practice is widely used to mechanically open the Eustachian tube, directly facilitating pressure relief and improving overall middle ear ventilation.
7. Softening Impacted Wax with Olive Oil
When water becomes securely trapped behind a dense wall of impacted earwax, the wax itself must be thoroughly treated before the fluid can successfully escape. You can safely apply a few drops of warmed, medical-grade olive oil or over-the-counter hydrogen peroxide directly into the ear canal while lying comfortably on your side 17. Allow the solution to remain undisturbed for several minutes to deeply penetrate and soften the impacted cerumen matrix. If utilizing hydrogen peroxide, the liquid will noticeably fizz and bubble as it actively releases oxygen, mechanically breaking apart the wax barrier. After resting, simply tilt your head to drain the mixed fluids. Because hydrogen peroxide eventually breaks down into water, you may need to follow up with a hair dryer to ensure the canal is left completely desiccated.
Note: This lubricating method is commonly used to safely dissolve stubborn cerumen impactions, thereby liberating any hidden fluids trapped firmly behind the waxy barrier.
Differentiating Outer Ear Water from Middle Ear Fluid
A critical diagnostic distinction must always be established between water trapped in the external ear canal (the space outside the eardrum) and fluid trapped within the middle ear (the cavity located directly behind the eardrum). While both conditions share frustratingly identical symptoms such as persistent aural fullness and muffled hearing their physical anatomical locations, underlying physiological causes, and mandated medical treatments are vastly different.
Moisture localized in the outer ear strictly represents an environmental intrusion. It originates from the outside world via recreational swimming, daily showering, or heavy perspiration, and is physically blocked from traveling any deeper by a healthy, intact eardrum. It is universally considered a quick, transient issue that is easily resolved through the mechanical gravity techniques or chemical drying methods detailed in standard care protocols.
Conversely, fluid accumulation in the middle ear is a complex, internal physiological issue entirely independent of swimming or bathing habits. This distinct condition is primarily driven by Eustachian tube dysfunction (ETD). The Eustachian tube acts as a vital biological pressure valve connecting the middle ear cavity to the back of the nasopharynx. Its designated role is to open briefly during swallowing or yawning to seamlessly equalize atmospheric pressure and drain natural mucosal secretions. If this narrow tube swells shut due to a viral cold, severe allergic rhinitis, sinus infections, or rapid barometric pressure changes (such as flying in a commercial airplane), the middle ear becomes entirely sealed off {% https://www.ncbi.nlm.nih.gov/books/NBK555908/ %}.
Once the Eustachian tube is obstructed, the ambient air trapped inside is slowly absorbed by the surrounding mucosal tissues, which inadvertently creates a negative pressure vacuum. This powerful vacuum physically retracts the eardrum inward and begins to siphon serous fluid from the surrounding vascular membranes directly into the middle ear space. Over time, this initially thin fluid can thicken into a remarkably sticky, mucus-like substance, a condition clinically documented as “glue ear” or otitis media with effusion 18. Because this thick fluid is securely trapped behind a solid eardrum, no amount of head tilting, rubbing alcohol drops, or external hair drying will successfully remove it. It generally requires the passage of time, systematic decongestants, or in severe, chronic cases, the surgical placement of tympanostomy tubes to artificially ventilate the sealed space 19.
| Clinical Feature | Outer Ear Water Retention | Middle Ear Fluid (Eustachian Tube Dysfunction) |
| Origin of the Fluid | External environment (swimming pools, showers, rain). | Internal bodily secretions (mucus, serous plasma fluid). |
| Anatomical Location | In the external auditory canal, directly in front of the eardrum. | In the middle ear cavity, completely enclosed behind the eardrum. |
| Primary Cause | Physical obstruction (swollen wax, anatomical isthmus) trapping water. | Inflammation and blockage of the Eustachian tube due to allergies or illness. |
| Associated Symptoms | Audible sloshing sound with head movement, possible localized itching. | Internal popping sounds when swallowing, history of recent cold or sinusitis. |
| Effective Removal Strategy | Gravity manipulation, alcohol/vinegar drops, thermal evaporation techniques. | Time, oral nasal decongestants, Valsalva maneuver, professional medical intervention. |
The Microbiological Risks of Retained Moisture
Diving deeply into the microscopic ecosystem of the ear canal clarifies precisely why prompt water removal is considered so medically vital. The surface of healthy external auditory canal skin naturally harbors a stable, entirely non-harmful population of various microbial species, prominently including Staphylococcus epidermidis and Corynebacterium species 6. These benign resident bacteria exist in a delicate symbiotic balance, largely kept in check by the robust acidic pH of natural cerumen and the inherently dry nature of the anatomical environment.
Disaster strikes when water is introduced and allowed to stagnate, acting as a potent catalyst for a drastic microbiological shift. The pooling water aggressively dilutes the protective enzymes and antimicrobial peptides that are naturally secreted by the ear’s specialized sebaceous glands. As the skin undergoes the process of maceration absorbing water until it becomes heavily wrinkled, soft, and highly permeable microscopic fissures develop throughout the epidermal layer 20. This compromised physical barrier suddenly becomes highly hospitable to a host of opportunistic environmental pathogens that inherently thrive in warm, aquatic conditions.
The most notorious and aggressive of these microscopic invaders is Pseudomonas aeruginosa, a virulent, gram-negative rod bacterium frequently isolated in damp soil, public swimming pools, and poorly maintained hot tubs. Pseudomonas is uniquely and perfectly adapted to flourish in the exact humid, slightly alkaline conditions generated by trapped shower water. Once it successfully colonizes the micro-fissures of the macerated ear canal, it secretes powerful exotoxins and destructive enzymes that trigger rapid, intensely painful tissue inflammation, universally characterizing the classic clinical presentation of acute otitis externa 21. Another remarkably common bacterial culprit is Staphylococcus aureus, which tends to incite localized, pus-filled infections such as painful furuncles or boils situated deep within the hair follicles of the outer cartilaginous canal.
Looking beyond bacterial threats, environmental fungi also pose a massive, often overlooked significant threat to the damp ear. Prolonged moisture exposure, particularly in excessively hot and humid geographic climates or following the inappropriate overuse of topical antibacterial drops, sets the ideal stage for otomycosis—a stubborn fungal infection of the ear canal. Aspergillus and Candida species represent the primary fungal pathogens directly responsible for this maddening condition 22. Fungal infections typically present with noticeably less acute pain than their bacterial counterparts but cause severe, relentless pruritus (itching) and produce a thick, cotton-like or violently discolored discharge. Therefore, actively and aggressively managing ear moisture is never merely a matter of simple physical comfort; it represents a critical preventative medical measure against aggressive microbial colonization.
Preventive Measures for Water Enthusiasts
For individuals who swim regularly, participate in high-intensity water aerobics, or simply happen to produce excess earwax that inherently traps daily shower water, implementing proactive prevention is vastly superior to seeking reactive treatment. Establishing a consistent, rigorous ear care routine both before and immediately after any water exposure significantly curtails the risk of fluid retention and subsequent infection.
Initiating a physical barrier protocol is highly recommended for all frequent swimmers. Wearing a tight-fitting silicone or latex swimming cap that covers the ears entirely serves as a simple, highly effective strategy to minimize bulk water entry into the canal 23. For much more targeted internal protection, obtaining custom-fitted swim molds or utilizing high-quality over-the-counter silicone earplugs creates a dependable waterproof seal directly at the opening of the ear. However, you must absolutely avoid standard foam earplugs in any aquatic setting, as they are highly porous, readily absorbing contaminated water and holding it directly against the ear canal lining. Alternatively, gently applying a small cotton ball lightly coated in petroleum jelly into the outer ear bowl just before showering acts as a highly effective, temporary hydrophobic barrier 24.
Cultivating disciplined post-exposure habits is equally crucial to long-term ear health. Establishing a routine of drying the ears thoroughly immediately after leaving the water represents the absolute best defense against the onset of otitis externa. Use the soft corner of a clean, dry towel to meticulously wipe only the outer visible rim of the ear. You must never shove the towel deep into the canal itself. Combining this external drying with the low-heat hair dryer method ensures that any microscopic droplets resting near the eardrum are safely evaporated before they can trigger skin maceration.
Implementing a prophylactic chemical approach is often recommended by physicians for individuals suffering from highly recurrent issues. Using commercial, alcohol-based swimmer’s ear drops immediately after finishing a swim routine quickly and efficiently desiccates any remaining moisture while simultaneously re-establishing the crucial acidic barrier 25. This incredibly simple, ten-second chemical reset is frequently all that is required to permanently break the vicious cycle of chronic water retention and painful outer ear infections, provided the individual possesses intact eardrums and lacks any underlying dermatological conditions affecting the ear.
Activities to Avoid When You have Trapped Water in the ear
When confronted with the maddening, distracting sensation of fluid trapped in the ear, human instinct often drives us to take immediate, sometimes dangerously aggressive action. Unfortunately, many common household practices do far more physical harm than good, severely exacerbating the problem or causing traumatic, irreversible injury to the ear’s delicate internal structures.
1. Inserting Cotton-Tipped Swabs
You must never insert cotton-tipped swabs, metal bobby pins, paperclips, keys, or even your own fingernails into the ear canal in a misguided attempt to soak up water or aggressively scrape out wax 26. While a dry cotton swab might absorb a tiny fraction of the surface water, its primary mechanical effect is to act precisely like a ramrod. It aggressively pushes surrounding earwax much deeper into the bony portion of the canal, packing it tightly against the eardrum and creating an impenetrable, water-logged plug. Furthermore, the coarse microscopic fibers of the cotton create painful abrasions (microtrauma) on the ultra-thin skin of the canal, providing ambient bacteria immediate, direct access to the underlying bloodstream and practically guaranteeing a painful infection.
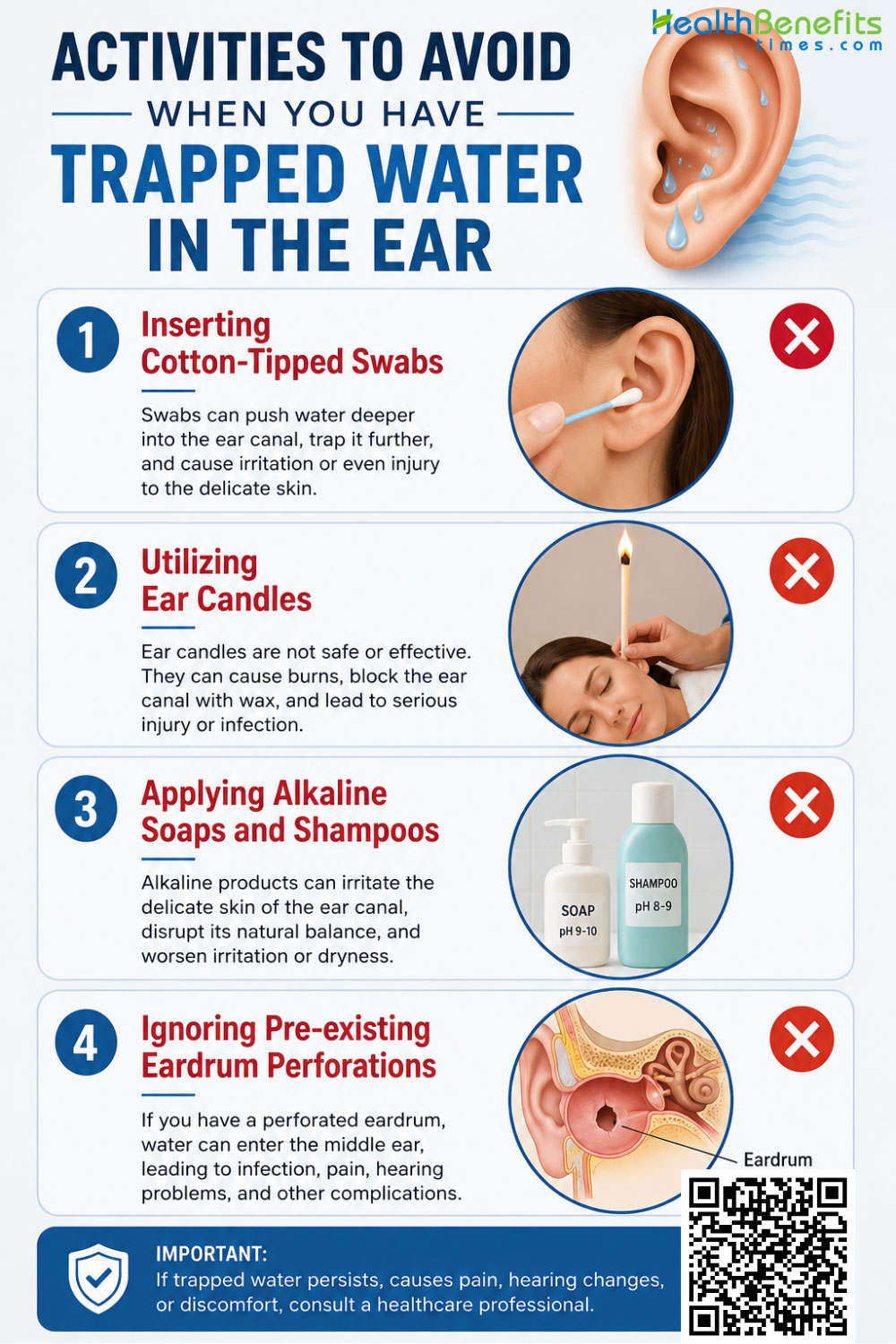
2. Utilizing Ear Candles
You should absolutely avoid the dangerous use of ear candles under all possible circumstances. The pseudoscientific practice of ear candling involves placing a hollow, cone-shaped wax candle directly into the ear canal and lighting the exposed end on fire, under the entirely false premise that the rising heat creates a vacuum to magically draw out wax and trapped moisture. Clinical medical studies have repeatedly and conclusively proven that ear candles do not generate any measurable vacuum whatsoever and are entirely ineffective at removing water or cerumen 15. Worse still, the practice introduces severe physical risks, including depositing scalding hot candle wax directly onto the eardrum, burning the facial skin or hair, and potentially puncturing the tympanic membrane.
3. Applying Alkaline Soaps and Shampoos
While taking a hot, relaxing shower, you might be strongly tempted to vigorously wash the inside of your ear with standard body soap or heavy shampoo to clear out the trapped water. You must avoid allowing these highly alkaline hygienic products to enter the deeper canal. The human ear relies heavily on its naturally acidic pH to continuously fend off bacterial and fungal growth. Introducing alkaline soaps instantly neutralizes this protective acid mantle, rapidly accelerating the breakdown of the skin barrier and significantly increasing your biological susceptibility to swimmer’s ear. To safely clean the outer ear, simply use a dry tissue or an alcohol-free baby wipe strictly on the external cartilaginous folds of the pinna after bathing 27.
4. Ignoring Pre-existing Eardrum Perforations
You must never arbitrarily use any liquid drops including over-the-counter drying agents, rubbing alcohol, acetic acid vinegar, or bubbling hydrogen peroxide if you have a known medical history of a ruptured (perforated) eardrum or if you currently have surgically implanted tympanostomy tubes (ear tubes) 28. In these specific clinical scenarios, the crucial physical barrier separating the outer and middle ear is completely absent. Introducing non-sterile or highly acidic liquids can allow these caustic substances to flood directly into the delicate middle ear space, causing agonizing, immediate pain, heavily damaging the tiny ossicle bones, and potentially leading to permanent sensorineural ototoxicity and profound hearing loss.
When to see Doctor
While the vast majority of instances involving trapped water can be safely and swiftly managed at home utilizing basic fluid dynamic principles and over-the-counter remedies, certain specific symptoms indicate that the situation has dangerously escalated beyond simple moisture retention. If the water has successfully triggered a severe bacterial or fungal infection, or if there is underlying structural damage to the ear’s anatomy, professional medical evaluation is absolutely mandatory to prevent permanent complications.
1. Escalating Pain or Severe Tenderness
You should seek immediate, professional medical attention if the mild, annoying discomfort in your ear rapidly transitions into sharp, severe, or relentless throbbing pain. A classic, hallmark sign of an advancing acute otitis externa infection is extreme, disproportionate tenderness when you gently pull on your earlobe or push inward on the tragus (the small, prominent flap of cartilage located just in front of the ear canal opening) 2. If manipulating the outer ear causes severe agony, the internal skin is actively inflamed and heavily infected, requiring specialized prescription antimicrobial drops to resolve.
2. Discolored or Foul-Smelling Otorrhea
You must consult a licensed healthcare provider if you notice any fluid draining from your ear that is distinctly yellow, green, excessively cloudy, or accompanied by a foul, pungent odor. Healthy water drainage is always clear, thin, and completely odorless. Purulent (pus-like) discharge strongly indicates a thriving, aggressive bacterial infection or a recently ruptured eardrum, while a thick, cottage-cheese-like white or black discharge is a classic clinical indicator of a fungal otomycosis infection that requires entirely different antifungal medications.
3. Systemic Symptoms and Fever
You need to visit a doctor promptly if your localized ear symptoms are accompanied by systemic, whole-body signs of illness. If you develop a sudden fever, experience whole-body chills, or notice that the lymph nodes located directly behind your ear or down the side of your neck have become noticeably swollen and highly tender to the touch, the localized ear infection has successfully breached the superficial tissues. This ominous development indicates the infection is actively spreading into the surrounding lymphatic system or deeper soft tissues, a serious medical condition that may require potent oral antibiotics to fully eradicate.
4. Prolonged Conductive Hearing Loss
You should arrange an immediate appointment with an otolaryngologist (ENT) if the feeling of deep fullness or significantly muffled hearing does not completely resolve within two to three days despite utilizing all safe home removal methods. Prolonged conductive hearing loss or the sudden, jarring onset of continuous tinnitus (ringing in the ear) strongly suggests that there may be severe, stone-like cerumen impaction plastered directly against the tympanic membrane, or that thick, viscous fluid has accumulated deeply in the middle ear space. Both of these specific scenarios require professional extraction using specialized microscopic suction equipment and long surgical tools 21.
5. Managing Surgical Implants or Prior Injuries
You must immediately bypass all home remedies and see a specialized physician if you get water trapped in your ear and you possess a known history of severe otologic conditions. This strictly includes individuals who currently have tympanostomy tubes actively in place, those who have previously suffered from a traumatic ruptured eardrum that has not fully healed, or individuals who have recently undergone highly specialized ear surgeries like a tympanoplasty or mastoidectomy 16. In these high-risk medical scenarios, introducing water or attempting to aggressively remove it incorrectly can easily lead to deep-seated, chronic suppurative otitis media and potentially permanent, irreversible auditory damage.