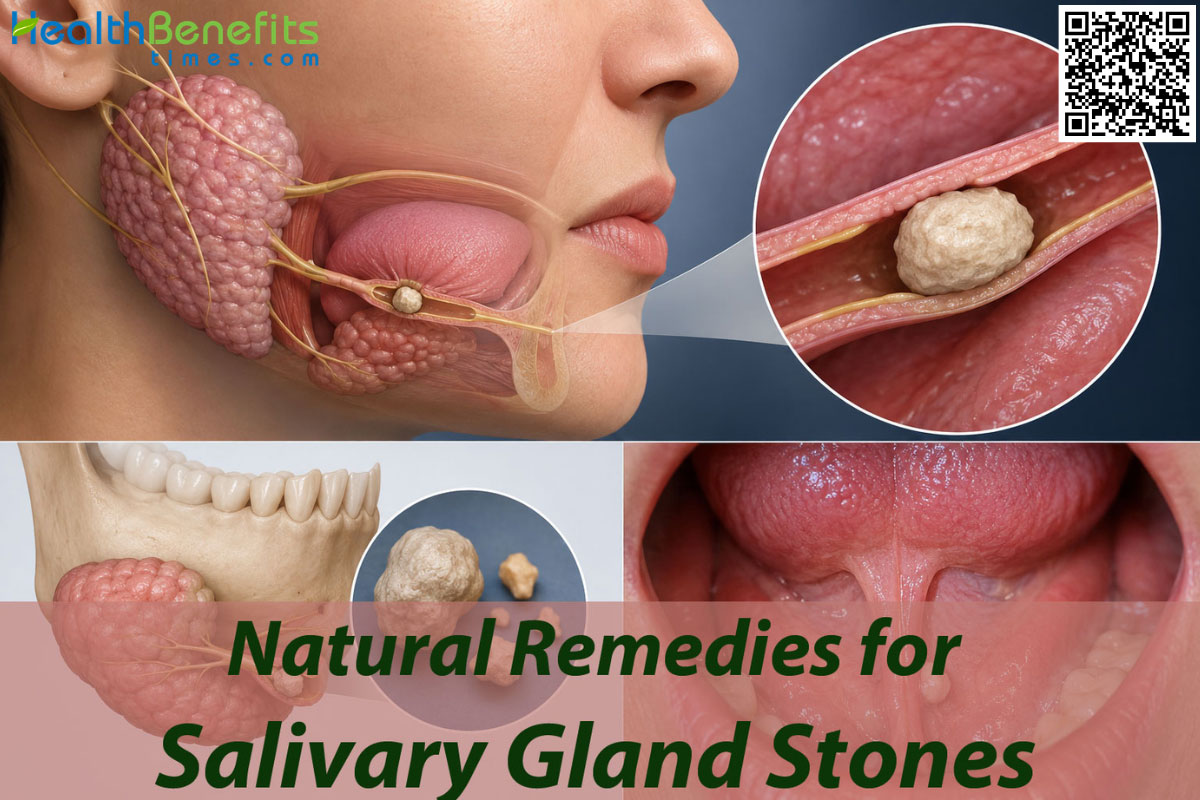
Salivary gland stones (medically known as sialolithiasis) are small, hardened mineral deposits primarily composed of crystallized calcium that form inside your salivary glands or the tiny tubes (ducts) that deliver saliva into your mouth. When these stones grow large enough, they act like a dam, partially or completely blocking the flow of saliva. Because your body naturally produces a surge of saliva when you eat or smell food, this blockage causes the fluid to back up. This buildup results in uncomfortable swelling, tenderness, and sharp or throbbing pain in your jaw, cheek, or neck, particularly during mealtimes. While the exact trigger isn’t always clear, the formation of these stones is heavily linked to dehydration, chronic dry mouth, and certain medications that reduce saliva production. Minor stones can often be naturally flushed out by staying hydrated and massaging the area, while larger ones may require minor medical procedures. 1, 2, 3.
Causes of Salivary Gland Stones
Exploring the exact origins of these glandular blockages reveals a remarkably complex interplay between human anatomical structures, daily lifestyle habits, and underlying cellular metabolic processes. The precise sequence of events that triggers the crystallization of saliva is not entirely singular; rather, it typically emerges from several distinct, overlapping contributing factors.
1. Anatomical Layout and Fluid Dynamics
The specific physical architecture of the human salivary network plays a critical, foundational role in stone formation. The submandibular gland, nestled deeply beneath the lower jawbone, serves as the most frequent site for these crystalline blockages, accounting for the vast majority of documented cases. This staggering prevalence is largely due to the unique trajectory of its primary excretory pathway, known as Wharton’s duct. This particular channel is exceptionally long, uniquely tortuous, and travels on an upward incline against the constant pull of gravity 4. Because the saliva must be physically pushed uphill to enter the floor of the mouth, natural physiological retention zones are created. Within these stagnant pockets, the fluid moves sluggishly, providing an ideal, undisturbed environment where microscopic mineral particles can settle, aggregate, and slowly precipitate into a solid mass over prolonged periods.
2. The Intrinsic Chemical Composition of Saliva
Beyond physical anatomy, the intrinsic biochemical makeup of the saliva itself is a powerful determining factor in the lithogenesis, or stone-creation, process. The submandibular gland is uniquely programmed to produce a specialized type of saliva that is notably more alkaline and significantly richer in calcium, phosphates, and heavy mucin proteins compared to the secretions of other glands. This thick, highly viscous fluid essentially acts as a chemical incubator. When the alkaline nature of the saliva interacts with its high mineral density, it creates a supersaturated environment. Calcium phosphates are naturally drawn to aggregate around microscopic organic debris, clustering together to solidify into a hard, calcified mass. This is in stark contrast to the parotid glands located in the cheeks, which secrete a much thinner, watery, serous fluid that is inherently less likely to stagnate and crystallize 5.
3. Underlying Systemic and Metabolic Conditions
Certain chronic health profiles quietly but substantially encourage the formation of salivary stones by altering the body’s overall internal chemistry. Rigorous epidemiological research indicates that broader metabolic and systemic issues serve as significant catalysts for glandular obstructions. Conditions such as severe dyslipidemia an imbalance of lipids and cholesterol in the bloodstream have been strongly correlated with a higher risk profile for developing these calcifications 6. Furthermore, individuals suffering from systemic obesity or autoimmune disorders like Sjögren’s syndrome, which actively diminishes natural saliva production, face exponentially increased odds of sialolithiasis due to severe, chronic ductal dryness 7. The presence of other systemic mineral imbalances, such as a documented medical history of kidney stones (nephrolithiasis) or gallstones (cholelithiasis), strongly suggests a generalized physiological tendency to form mineral concretions throughout various organ systems 8.
4. Dehydration and Chronic Fluid Imbalance
A persistent lack of adequate bodily hydration acts as a primary, immediate trigger for accelerating stone development. When overall systemic water intake drops below optimal levels, the body aggressively conserves moisture, leading to a drastic decrease in total saliva volume while simultaneously increasing its relative thickness. This highly concentrated state acts as a multiplier for stone growth. As the fluid becomes denser, the relative distance between floating mineral salts decreases, accelerating their inevitable collision and crystallization. Therefore, prolonged periods of dehydration rapidly transform a harmless microscopic calcification into a clinically significant obstruction.
5. Microscopic Foreign Bodies and Local Inflammation
An imbalance in the localized environment of the mouth can inadvertently trigger a chain reaction resulting in mineral precipitation. Minor local infections, the retrograde ascent of oral bacteria into the duct opening, or the accidental introduction of microscopic foreign bodies can fundamentally disrupt the gland’s delicate equilibrium. These tiny intruders, which can include stray food particles or shed epithelial cells, act as an organic “nidus” or core. Once this core is established within the duct, the immune system triggers mild local inflammation, altering the surrounding pH. This chemical shift prompts the heavy mucins and calcium salts to rapidly layer themselves concentrically over the foreign core, building the stone layer by layer 9.
Symptoms of Salivary Gland Stones
Recognizing the active presence of a salivary blockage usually occurs during highly specific, predictable moments tied to the body’s digestive rhythms. The clinical signs are distinctly characteristic, rarely subtle, and are intimately connected to the autonomic nervous system’s response to food.
1. Sudden Meal-Time Pain
The absolute hallmark symptom of this condition is a sharp, distinct, and sometimes throbbing pain that predictably surges just before, during, or immediately after consuming a meal. As the brain anticipates the arrival of food, it commands the salivary glands to rapidly produce and excrete a massive volume of saliva. This sudden surge of fluid rushes forcefully down the duct but violently impacts the rigid stone wall, causing sudden, intense hydrostatic pressure and subsequent acute pain within the gland itself 10.
2. Intermittent Glandular Swelling
Accompanying the classic meal-time pain is a highly noticeable, localized swelling in the affected anatomical area. Depending on the stone’s location, a sudden lump may appear prominently under the jawline (submandibular) or in front of the earlobe and along the cheek (parotid). This swelling typically reaches its absolute peak during active mastication and then slowly, agonizingly subsides over the following hours as the trapped saliva gradually seeps out around the edges of the partial obstruction 11.
3. A Tender, Palpable Mass
In a significant number of instances, a firm, highly tender lump can be physically felt by running a finger under the jawline or pressing gently along the soft tissue of the mouth’s floor. This firm mass is either the engorged, inflamed salivary gland itself protesting the pressure, or it is the physical calcified stone resting palpably near the very exit orifice of the duct.
4. Altered Oral Sensation and Dryness
A persistent, slightly foul or metallic taste might linger chronically in the mouth if old, stagnant saliva has been trapped behind a stone for days. Additionally, patients frequently report that the affected side of their mouth feels unusually parched or dry, as the primary source of lubricating moisture has been effectively dammed up.
5. Warning Signs of Bacterial Infection
If the mechanical obstruction becomes severe, absolute, and chronic, the bacteria naturally trapped in the stagnant pool of saliva can multiply at a staggering rate. This dangerous escalation, known as acute suppurative sialadenitis, manifests as rapidly worsening, unremitting pain, the visible discharge of foul-tasting pus into the oral cavity, severe localized redness, and potentially the onset of a systemic low-grade fever 12.
Salivary Gland Stones Facts
Grasping the broader statistical and clinical context of this condition helps immensely in demystifying the patient experience. The following table provides a meticulously categorized, comprehensive overview of the fundamental facts surrounding salivary gland stones.
| Category | Details |
| Symptoms |
|
| Causes |
|
| Types of Salivary Gland Stones 13. |
|
| How does spread |
|
| Age Group 14. |
|
| You might be at a higher risk for exposure of this disease if you: |
|
| How doctors diagnose 16 |
|
| Other facts |
|
Natural Remedies for Salivary Gland Stones
Navigating the early, incredibly frustrating stages of a salivary blockage often involves utilizing simple, entirely non-invasive techniques aimed squarely at encouraging the human body to naturally dislodge and expel the stone. Conservative care is exceptionally effective for smaller calcifications and strictly focuses on supercharging saliva production, physically relaxing the ductal walls, and gently coaxing the obstruction out of its resting place.
1. Focused Hydration Therapy
Water acts as the primary, most vital vehicle for recovery in almost all benign glandular blockages. When you consciously and significantly increase your daily fluid intake, you fundamentally alter and thin out the overall biochemical consistency of your saliva. By ensuring the body exists in a state of mild hyper-hydration, the salivary glands are chemically forced to abandon the production of thick, mucin-heavy trickle and instead output a constant, highly watery stream of fluid. This non-stop hydrostatic pressure safely builds up behind the lodged stone, gently but persistently pushing the calculus forward millimeter by millimeter toward the tiny exit orifice of the duct 17. Proper hydration also ensures that the delicate mucous membranes lining the duct remain incredibly slick, vastly reducing internal friction that might otherwise anchor the stone in place.
Note: To utilize this natural remedy effectively, continuously sip room-temperature purified water throughout your entire day, aiming to drink enough so that your urine remains entirely clear, thereby facilitating the natural, frictionless flushing of the obstruction.

2. Citrus and Natural Sialagogues
Substances that provoke a massive, immediate salivary response are known within the medical field as sialagogues. Purposefully incorporating intensely sour items into your daily routine forces the affected gland into physiological overdrive. When you consume natural items that are heavily rich in citric or lactic acid, your brain instantly perceives a massive chemical stimulus on the tongue. In defense, the autonomic nervous system commands an immediate, forceful release of saliva to dilute the perceived acid. This sudden, violent flood of fluid can create enough sudden back-pressure to aggressively dislodge a stubborn stone that has adhered to the duct wall. Research has highlighted that natural, highly acidic options ranging from a raw slice of lemon or pure lemon juice to a surprisingly effective splash of malt vinegar produce the absolute highest volume of salivary flow available without pharmaceutical intervention 18.
Note: These natural acidic stimulants are most commonly eaten, sipped, or sucked on directly before or actively during meals to purposefully maximize sudden saliva production and vigorously flush the duct naturally.
3. Sustained Warm Compresses
Heat is an ancient, universal, and highly effective remedy for deep tissue relaxation and localized pain management. Applying a warm, moist towel directly to the external skin positioned over the swollen, angry gland serves a vital dual physiological purpose. First, the deep thermal energy drastically increases local capillary blood circulation, which helps dial down the immediate, painful inflammatory response and deeply soothes aching, cramped muscle tissues. Second, and more importantly for stone clearance, the sustained radiant heat actively helps to mildly relax and dilate the smooth muscle fibers wrapped around the delicate walls of the salivary duct. A slightly wider, relaxed duct means the rigid stone is afforded a slightly larger channel to travel through, significantly reducing internal friction, preventing painful spasms, and speeding up the natural expulsion process 19.
Note: This soothing remedy is commonly applied externally to the skin directly over the swollen cheek or jaw area for 15 to 20 straight minutes, repeated several times a day, to actively ease discomfort and dilate the passageway.
4. Hard Sour Candies and Lozenges
While perhaps not considered a traditional “herbal” remedy, hard sour candies serve an undeniable, historically proven therapeutic function in glandular care. Specifically, hard boiled sweets, intense lemon drops, and sherbet-flavored lozenges brilliantly combine the continuous mechanical action of sucking with the potent chemical stimulation of concentrated citric acid 20. The prolonged, unhurried presence of the candy dissolving slowly in the mouth ensures a sustained, steady, and unrelenting flow of saliva over an extended period. This persistent, gentle pressure is sometimes much more effective at slowly shifting a large stone than a single, rapid, violent burst of liquid that might simply cause immediate pain without moving the obstruction.
Note: These candies are meant to be consumed slowly, allowing them to dissolve completely in the mouth without chewing, to purposefully maintain a steady, therapeutic, and prolonged stream of saliva for medicinal clearance.
5. Specialized Herbal Decoctions for Moisture
In cases where the salivary stone is a direct secondary result of chronic, unrelenting dry mouth, turning to carefully formulated herbal remedies can provide significant relief by restoring the body’s natural moisture balance. In various traditional medical systems, particularly Chinese medicine, specific combinations of herbs are utilized strictly as “Yin-nourishing” and “Body fluid-regenerating” agents. These specialized botanical decoctions are designed not just to mask dry mouth, but to actively stimulate the glandular parenchyma to resume normal secretory functions over time, thereby preventing the thick, stagnant conditions that originally allowed the stone to crystallize and mature 21.
Note: These formulated herbal remedies are commonly consumed as warm, steeped teas or daily liquid decoctions to systematically treat chronic dry mouth from within, thereby preventing the highly concentrated saliva that causes stones.
Is there any exercise or physical activities for Salivary gland stones?
Physical manipulation and targeted movement of the affected anatomical area can be incredibly beneficial when performed with caution. When executed carefully, highly specific manual exercises and physical stretching therapies can mechanically advance the stone forward and prevent the surrounding facial muscles from painfully cramping around the irritated, swollen gland.\
1. Salivary Gland Massage (Milking the Duct)
This is a highly deliberate, tactile technique designed to physically and manually push the solid obstruction forward through the delicate tube. Because the primary salivary ducts run incredibly close to the surface of the mouth’s soft floor and the inner cheek lining, external and targeted internal pressure can safely guide the stone. The primary goal is to begin palpating just behind where the deepest swelling is felt, and then apply firm, rolling, forward pressure moving precisely toward the tiny opening of the duct located under the tongue or near the upper teeth. This specific rolling action mimics the natural forward movement of fluid, creates an artificial wave of pressure, and actively helps break any stubborn, sticky mucous seals that might be rigidly holding the stone in its place 22.
Note: To do this correctly, use two meticulously clean fingers to apply gentle but firm pressure starting near the back angle of your jaw or the rear of your cheek, slowly and deliberately rolling your fingers forward toward your front teeth immediately after a meal when the duct is visibly full of fluid.
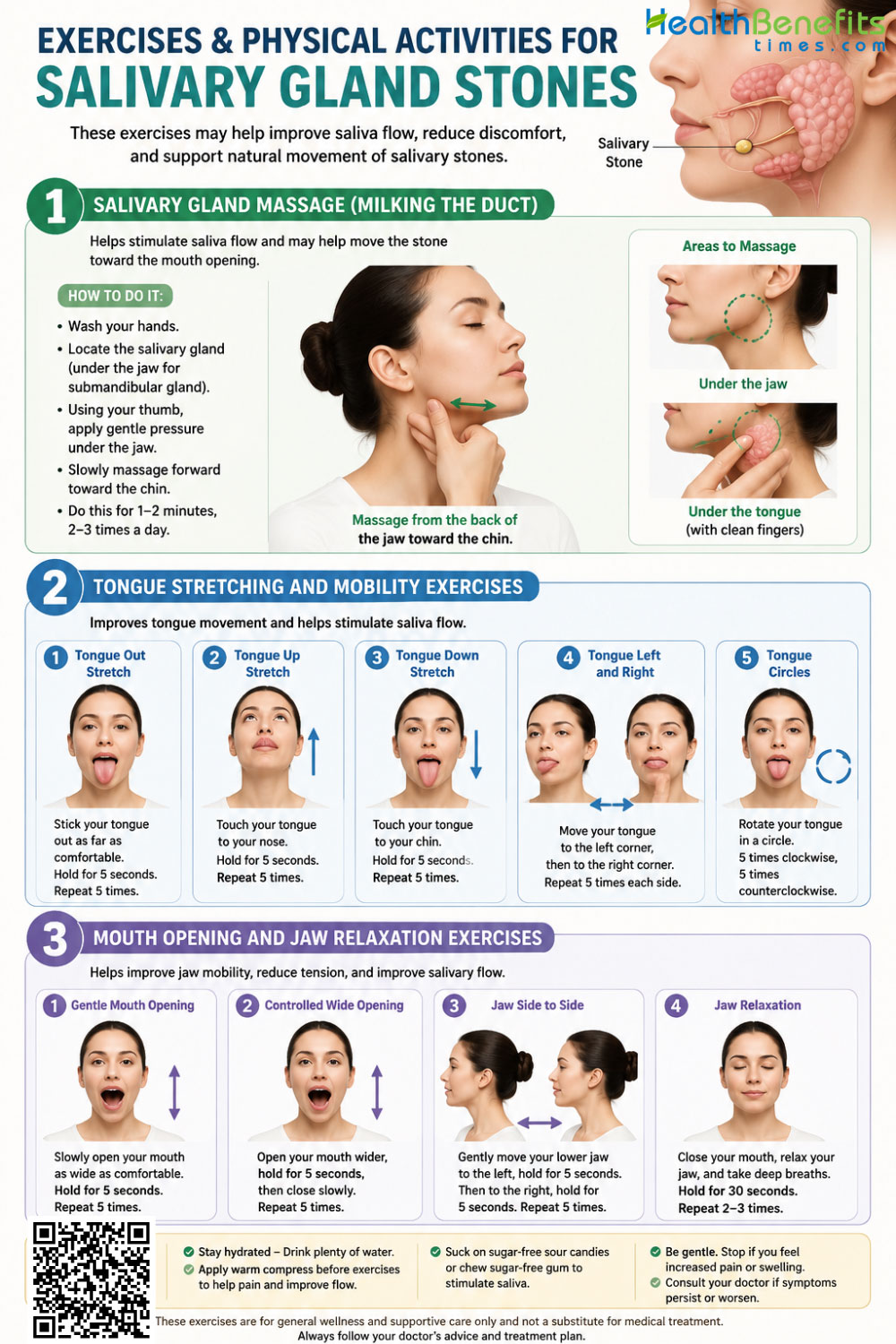
2. Tongue Stretching and Mobility Exercises
The crucial submandibular ducts lie buried directly beneath the muscular base of the tongue, and any resting tension in this complex area can severely restrict the duct’s natural flexibility and width. By consciously engaging in active, exaggerated tongue movements, you physically stretch the mucosal lining and the deep muscular floor of the mouth. This deep internal stretching can subtly, temporarily alter the physical angle of the duct, sometimes providing just enough geometric shift to allow a tightly wedged, angled stone to break free and shift its position toward the exit 23.
Note: To perform this stretch, push the flat of your tongue incredibly firmly against the hard roof of your mouth, hold the extreme tension for several seconds, and then stretch it out and down as far as possible toward your chin, repeating this full cycle gently ten times a day.
3. Mouth Opening and Jaw Relaxation Exercises
A severely swollen, throbbing salivary gland almost always leads to secondary, highly painful jaw stiffness, as patients subconsciously restrict their facial movements to avoid triggering sharp pain. Deliberate, gentle mouth-opening exercises actively prevent the massive jaw muscles, specifically the powerful masseter, from tightening up and going into spasm. Keeping the structural jaw completely relaxed ensures that the surrounding dense tissues do not place any additional, agonizing compressive force directly onto the swollen, hyper-sensitive gland 24.
Note: To execute this safely, slowly open your mouth as wide as comfortably possible without causing a sharp spike in pain, hold the maximum stretch steadily for five full seconds, and then slowly close; perform this gentle stretch a few times in succession, particularly after applying a soothing warm compress to the area.
Foods and Activities to Avoid
When you are actively managing a painful salivary blockage, making incorrect choices can inadvertently worsen the internal pressure, severely dry out the oral cavity, or massively increase your pain levels. Adjusting your daily intake habits temporarily is absolutely crucial for ensuring a smooth, complication-free recovery.
Foods to Avoid When You Suffer from Salivary Gland Stones
1. Extremely Dry or Absorbent Foods
Items such as dense crackers, dry toast, and thick, unmoistened breads require massive, immediate amounts of saliva to chew, soften, and swallow safely. Attempting to process these highly absorbent foods forces a severely blocked gland to work exceptionally hard against a closed door, leading to rapid, agonizing swelling without providing any fluid relief to the digestive tract.

2. Dehydrating Beverages (Caffeine and Alcohol)
Heavy coffee, strong black tea, and concentrated energy drinks act as mild systemic diuretics, directly contributing to unwanted cellular dehydration. Furthermore, caffeine often leaves the mouth feeling instantly dry and highly astringent, thickening the resting saliva and making it exponentially harder for the gland to naturally flush out a stone. Similarly, alcoholic spirits severely draw moisture out of the delicate oral tissues, diminishing overall fluid volume and slowing down all natural physiological healing mechanisms.
3. Massive, Complex Meals
Sitting down to eat a massive, multi-course meal triggers a prolonged, overwhelming, and intense salivary response from the brain. If a duct is completely structurally blocked, this massive, unyielding demand for fluid will rapidly cause severe, throbbing, unbearable pain. It is infinitely better to consume very small, highly frequent, soft, and moist meals to manage the glandular pressure safely and comfortably throughout the day.
4. Strictly Low-Protein, Non-Acidic Diets
Interestingly, to prevent future stone formation once an obstruction is cleared, avoiding a completely bland diet is recommended. Clinical observations note that maintaining a diet that is adequately rich in proteins and explicitly includes healthy acidic foods and liquids is actually highly advisable, as this specific nutritional profile constantly stimulates healthy flow and prevents the exact stagnation that leads to new sialolith formation 25.
Activities to Avoid When You Suffer from Salivary Gland Stones
1. Strenuous Exercise Without Aggressive Hydration
Engaging in heavy, sweat-inducing cardiovascular workouts, intense weightlifting, or spending prolonged time in a hot sauna leads to significant, rapid fluid loss through the skin. If this critical fluid is not immediately and continuously replaced with water, your remaining saliva will rapidly thicken into a paste-like consistency, potentially turning a small, easily passable stone into a massive, stubborn, immovable blockage 26.

2. Ignoring a Pristine Oral Hygiene Routine
Skipping regular brushing, failing to floss, or avoiding mouthwash allows opportunistic oral bacteria to thrive and multiply rapidly. Because a blocked duct means significantly less saliva is available to naturally wash away daily microscopic debris, the risk of a secondary, highly dangerous bacterial infection traveling backward up the stagnant duct increases drastically if the mouth is not kept in a pristine state.
3. Aggressive, Non-Nutritive Chewing Habits
Mindlessly chewing on hard, non-food items like solid ice cubes, plastic pens, or even incredibly tough cuts of jerky forces the massive jaw muscles to contract forcefully and repeatedly around the highly swollen, tender gland. This unnecessary, repetitive physical trauma can severely aggravate the localized inflammation, turning a dull, manageable ache into a sharp, persistent, radiating pain.
Myths and Misconceptions
Medical conditions that manifest with sudden, highly unusual localized symptoms frequently attract cultural folklore and entirely incorrect anatomical assumptions. Clarifying these widespread misunderstandings ensures that patient interventions are based firmly on actual human physiology rather than unverified rumor.
| Myth | Reality |
| “Drinking too much milk or taking daily calcium supplements directly causes salivary stones to form.” 27 | Despite the undisputed fact that these stones are primarily constructed of calcified calcium phosphates, dietary calcium intake is absolutely not the primary biological driver. The stones form due to localized fluid stagnation, chronic bodily dehydration, and altered physical duct anatomy, not simply from eating dairy products or taking standard daily vitamins. |
| “Only the very elderly and frail experience salivary gland stones.” {% https://pmc.ncbi.nlm.nih.gov/articles/PMC3485463/ %} | This is a massive, widely held epidemiological misconception. While the elderly certainly can experience medication-induced dry mouth, the absolute peak statistical incidence for salivary stones actually occurs in younger to healthy middle-aged adults, typically striking those solidly between the ages of 30 and 60 years old. |
| “Salivary gland stones are identical in nature and cause to kidney stones.” | While both painful conditions involve unwanted mineral precipitation, they are biologically, chemically, and anatomically distinct. Salivary stones consist mainly of localized calcium phosphate driven by oral pH environments, whereas kidney stones involve complex oxalates or uric acid processed systemically through the renal system. Having one does not clinically guarantee the other. |
| “If the intense pain suddenly stops completely, the stone has successfully vanished.” 28 | A sudden, welcome cessation of acute pain frequently just means the massive buildup of trapped saliva has finally managed to leak slowly past the edges of the stone, temporarily relieving the extreme hydrostatic pressure. The physical stone itself may still be firmly lodged deep in the duct. Recurrent swelling is highly common until the stone is truly, physically expelled into the mouth. |
| “You need to rush into immediate, invasive surgery the moment a stone is discovered.” | The overwhelming majority of small to medium salivary stones can be managed highly successfully with patient, conservative therapies like targeted massage, hyper-hydration, and potent sialagogues. Invasive surgical excision is usually strictly reserved only for giant, stubborn stones that repeatedly fail all safe, non-invasive treatments over a prolonged period. |
| “Children are just as likely as adults to get salivary stones from poor diets.” 29 | Pediatric salivary stones are exceptionally rare clinical anomalies. The overall incidence in global pediatric populations is extremely low, accounting for a mere 3% of all documented sialolithiasis cases, making it highly unlikely that a child’s sudden swelling is a stone without other major ruling-out diagnoses. |
Special Considerations
The medical approach to safely managing a salivary obstruction must seamlessly adapt to the vastly different, unique physiological states of various individuals. Age, underlying systemic health, and temporary, massive hormonal life phases all deeply influence how this exact condition behaves and how it must be carefully treated.
1. Children
The occurrence of true salivary stones within the pediatric population is incredibly, statistically rare, representing a minute fraction of overall documented clinical cases. Because it is so uncommonly seen, a young child presenting with sudden, painful swelling under the jaw is significantly more likely to be evaluated first for highly contagious viral infections like the mumps or massively swollen, reactive lymph nodes before a calcified stone is ever officially suspected 30. When a confirmed stone does stubbornly occur in a child, pediatricians almost exclusively mandate the gentlest, most conservative measures available aggressive oral hydration, warm soothing compresses, and safe, weight-based analgesics strictly avoiding any invasive surgical procedures unless the child faces a severe, life-altering complication.
2. Pregnancy
During the nine months of pregnancy, the human body undergoes massive, systemic fluid shifts, wildly fluctuating hormonal levels, and notable changes in resting oral pH. Many pregnant individuals suffer through prolonged periods of morning sickness, which can rapidly lead to severe temporary dehydration and a highly acidic, highly irritated oral environment. This perfect storm creates a theoretical biological predisposition for thicker, more viscous resting saliva. If a painful stone develops during a pregnancy, clinical management relies entirely and exclusively on natural, non-invasive home remedies like vastly increased water intake and mild glandular massage. This is because standard surgical interventions, heavy anesthetics, and potent prescription medications are generally strictly postponed to fiercely protect both maternal stability and fetal development.
3. Chronic Conditions
Individuals actively battling long-term, systemic metabolic or autoimmune diseases very often experience salivary stones as a highly frustrating, secondary medical complication. Autoimmune conditions like Sjögren’s syndrome inherently and aggressively attack the body’s moisture-producing glands, resulting in chronically low, incredibly thick saliva that is highly prone to rapid calcification. Similarly, metabolic disorders such as chronic gout fundamentally alter the chemical balance of bodily fluids, potentially predisposing the patient to unique stones composed primarily of uric acid rather than standard calcium 31. For these deeply complex patients, simply treating the isolated stone is only a temporary, fleeting fix; aggressively managing the underlying chronic disease with specialists is absolutely mandatory to prevent continuous, painful recurrence.
4. Elderly
Advanced age brings a deeply unique, often highly complicated set of challenges regarding daily oral health and fluid dynamics. The elderly demographic frequently relies on taking multiple daily prescription medications ranging from complex blood pressure pills to necessary antidepressants many of which explicitly list severe dry mouth (xerostomia) as a primary, unavoidable side effect 32. This chemically induced, chronic lack of thin saliva makes older adults highly, continuously susceptible to both initial stone formation and devastating secondary bacterial duct infections. Care for older adults must rigorously involve a careful, holistic review of their entire pharmaceutical regimen by a physician, alongside heavily encouraging the constant, daily sipping of water to forcibly maintain a safe, functional level of oral moisture.
Precaution Before Use of Natural Remedies When You Have Salivary Gland Stones
Taking proactive charge of your physical recovery using natural, home-based methods is incredibly empowering, but it must absolutely be done with a deep respect and understanding of the human body’s fragile limits. Overzealous, aggressive application of these home therapies can sometimes trigger vastly more physiological harm than good if you do not respect the condition’s absolute boundaries.
- Do Not Vigorously Massage an Actively Infected Gland: If the external skin resting over the gland is bright, angry red, physically hot to the touch, and you are experiencing a rising fever, you must cease all physical massage immediately. Blindly milking an actively infected, pus-filled gland can violently push live bacteria deeper into the surrounding pristine facial tissues, potentially causing a severe, rapidly spreading, life-threatening abscess 33.
- Carefully Regulate the Intake of Sour Foods: While pure lemon juice and intense sour candies are unparalleled for rapidly stimulating saliva, continuously consuming massive, unchecked amounts of potent citric acid can rapidly and permanently erode your protective dental enamel. Ensure you proactively rinse your mouth with plain, neutral water immediately after using strong sour stimuli to actively protect the long-term structural integrity of your teeth.
- Always Test the Temperature of Warm Compresses: The delicate skin on the human neck and face is highly sensitive to thermal damage. Always physically test a fresh, warm compress on the inside of your wrist for several seconds before blindly applying it to your jaw. An overly scalding towel will absolutely not heal the internal duct any faster, but it can easily and quickly cause painful, blistering surface burns right on top of your existing, throbbing glandular pain.
- Pace the Saliva Stimulation Carefully: If you apply a potent sour candy to your tongue and instantly experience sudden, blinding, excruciating localized pain, spit the candy out immediately. This violent reaction indicates the duct is 100% structurally blocked, and the rapid, massive influx of fresh saliva has literally nowhere to go. In cases of a total, unyielding blockade, extreme chemical stimulation will only cause pure agony rather than magically clearing the stone.
- Avoid Using Sharp Objects at All Costs: Under no circumstances should you ever attempt to physically dig out a partially visible stone with household tweezers, sharp toothpicks, or other unsterilized items. The mucosal tissue of the salivary duct is incredibly fragile, and amateur self-instrumentation easily causes deep lacerations, heavy, uncontrollable bleeding, and severe scar tissue formation that can permanently ruin the duct’s ability to function.
When to See a Doctor
While conservative, natural care is the absolute best first line of physiological defense, certain severe warning signs indicate that natural remedies are simply no longer sufficient to protect your health. Recognizing precisely when to transition away from home care and seek immediate, professional medical intervention is absolutely critical for preserving the long-term health and function of the salivary gland.
- The Unmistakable Presence of Pus: If you ever notice a distinctly foul-tasting, cloudy yellowish or greenish discharge actively leaking into your mouth from under the tongue or the side of the cheek, this is a definitive, undeniable sign of an active, dangerous bacterial infection that absolutely requires potent prescription antibiotics.
- Systemic Fever and Chills: A benign, localized mechanical blockage should never cause a full-body fever. If you suddenly develop a highly elevated temperature or begin experiencing uncontrollable, shaking chills, the localized inflammation has dangerously escalated into a systemic, full-body immune response, demanding immediate, emergency medical evaluation.
- Unrelenting, Severe, Disabling Pain: Pain that simply does not subside hours after a meal has ended, or a level of pain that entirely prevents you from sleeping, eating normally, or opening your mouth entirely, strongly indicates a severe, physical complication that requires a doctor’s immediate, targeted pain management and intervention.
- Swelling that Spreads Dangerously: If the initial swelling located strictly under your jaw rapidly expands downward into your neck, visually affects your physical ability to breathe, or noticeably alters the sound of your voice, you must seek emergency medical care immediately, as this suggests a highly dangerous, rapidly spreading deep tissue infection that could threaten your airway.
- Failure of the Stone to Pass After Weeks: If you have diligently and perfectly applied massive hydration, targeted massage, and warm compresses for several consecutive weeks and the hard, painful lump remains entirely unchanged, you must consult an otolaryngologist (ENT). Prolonged, unyielding blockage, even if it is only mildly painful, can steadily lead to permanent, irreversible glandular atrophy and the total destruction of the affected salivary gland over time 34. If conservative measures fail, these specialists can offer brilliant, minimally invasive modern procedures, such as laser lithotripsy or sialendoscopy, to safely and permanently fragment the stubborn stone without losing the gland 35.