Mouth breathing is exactly what it sounds like: the habit of inhaling and exhaling primarily through the mouth rather than the nose. While it is completely normal to breathe through your mouth during heavy exercise or a temporary cold, chronic mouth breathing is medically recognized as a symptom of an underlying obstructionIt typically happens when the nasal passages are partially or completely blocked by chronic allergies, a deviated septum, or enlarged tonsils and adenoids. The nose naturally filters, warms, and humidifies the air we breathe to protect our lungs. The mouth cannot perform these functions effectively, so relying on it for respiration causes physical complications over time. If left untreated, chronic mouth breathing can lead to a chronically dry mouth, bad breath, an increased risk of dental cavities, sleep disturbances like snoring or sleep apnea, and even developmental changes in a child’s facial structure. 1, 2.
Causes of Mouth Breathing
Unraveling why an individual instinctively opens their mouth to draw breath requires looking significantly beyond simple habits to investigate the underlying anatomy, tissue pathology, and immune responses of the upper respiratory tract. The etiology is profoundly multifaceted, frequently involving a complex combination of structural anomalies, inflammatory cascades, and neuromuscular deficits.
1. Adenoid and Tonsillar Hypertrophy
Enlargement of the lymphoid tissues situated at the back of the nasal cavity and throat serves as a leading driver of upper airway obstruction, particularly in pediatric populations. When adenoids become excessively large often due to recurrent viral infections, environmental irritants, or localized immune hyperactivity they physically barricade the aerial column of the nasopharynx. This dense tissue expansion drastically reduces the volume of air that can pass through the choanae, forcing the individual to seek an alternative, lower-resistance route for oxygen by opening the jaw 3.
2. Allergic Rhinitis
Chronic inflammation of the delicate mucosal lining within the nasal passages frequently triggers severe, unrelenting congestion. In response to inhaled environmental allergens such as tree pollen, dust mites, or animal dander, the immune system orchestrates an immunoglobulin E (IgE)-mediated inflammatory cascade. This biochemical response prompts mast cells to release histamine, which immediately engorges the nasal turbinates with fluid and exponentially increases thick mucus production, effectively shutting down the natural nasal airflow pathway 4.
3. Deviated Nasal Septum
A structural misalignment of the central cartilage and bone dividing the nasal cavity can drastically reduce the cross-sectional area of one or both nostrils. This asymmetrical narrowing creates a highly turbulent, high-resistance airflow environment inside the nose. Because the physics of fluid dynamics dictate that air will follow the path of least resistance, breathing through a severely deviated septum becomes physically exhausting, rendering natural nasal respiration entirely impossible without eventual surgical correction 5.
4. Orofacial Myofunctional Disorders (OMDs)
Weakness, imbalance, or flaccidity in the muscles of the face, particularly the lips (orbicularis oris) and cheeks (buccinator), can profoundly compromise the body’s ability to maintain a natural, resting lip seal. When these perioral muscles lack the necessary resting baseline tone, the mandible naturally drops open under the influence of gravity. This muscular failure allows for passive, continuous oral respiration throughout the day and night, even in the complete absence of any physical or inflammatory nasal blockage 6.
5. Ankyloglossia (Tongue-Tie)
Restricted mobility of the tongue, caused by a congenitally short, thick, or tight lingual frenulum, prevents the tongue from resting properly against the hard palate. Because the tongue remains anchored to the floor of the mouth, it completely fails to provide the internal structural scaffolding required to support the upper jaw and keep the mouth closed. This mechanical restriction leads to a cascade of compensatory mechanisms, including chronic mouth opening, improper swallowing patterns, and forward head posturing 7.
6. Functional Mouth Breathing Habituation
Perhaps one of the most clinically frustrating causes of oral respiration occurs when the original physical obstruction has been fully resolved, yet the breathing pattern persists. Following the surgical removal of enlarged adenoids or the successful medical management of severe allergies, the neuromuscular system may simply retain the deeply ingrained muscle memory of breathing through the mouth. Without active physical therapy and conscious retraining, the brain continues to default to the oral airway out of pure habit 5.
Symptoms of Mouth Breathing
Identifying a chronic oral breathing habit is clinically straightforward once the subtle and obvious signs that manifest across different anatomical systems are understood. Because the mouth is fundamentally not designed to filter, warm, or humidify inspired air, chronic exposure to raw environmental air triggers a highly distinct and predictable set of clinical symptoms.
- Physical and Facial Skeletal Signs:
- Development of an elongated, disproportionately narrow facial structure, clinically termed adenoidal facies or “long face syndrome” 8.
- A high, narrow, and distinctly V-shaped palatal arch resulting from the absence of upward tongue pressure.
- Severe dental malocclusions, most notably an anterior open bite (where the front teeth fail to touch) or a posterior crossbite 9.
- Chronic gingivitis and generalized inflammation of the upper anterior gums, driven largely by constant tissue dehydration and disrupted salivary protection.
- Noticeable forward head posture, an unconscious anatomical adaptation used to artificially widen and straighten a restricted airway.
- Systemic and Behavioral Symptoms:
- Chronic daytime fatigue, lethargy, and excessive sleepiness, stemming directly from fragmented, low-quality nighttime sleep architecture.
- Nocturnal snoring, audible gasping, and frequent micro-arousals that prevent the brain from reaching deep, restorative sleep stages 10.
- Episodes of nocturnal enuresis (bedwetting) in children, intricately linked to altered sleep stages and subsequent disruptions in antidiuretic hormone secretion.
- Behavioral challenges closely resembling Attention-Deficit/Hyperactivity Disorder (ADHD), driven by chronic intermittent hypoxia and sleep deprivation.
- Frequent, unexplained morning headaches resulting from poor overnight oxygenation and altered carbon dioxide exchange.
- Oral and Functional Disorders:
- Persistent dry mouth (xerostomia) immediately upon waking in the morning.
- Noticeable pooling of saliva or drooling on pillows during sleep.
- Speech sound disorders, particularly frontal or lateral lisps affecting the crisp pronunciation of sibilant consonants like /s/ and /z/ 11.
- Difficulty swallowing solid foods comfortably, often requiring an abnormal tongue thrust and a liquid wash to successfully clear the throat.
- Chronic halitosis (bad breath) resulting from an imbalanced, overly acidic oral microbiome that thrives in a dehydrated environment.
Mouth Breathing Facts
Visualizing the clinical realities and statistical prevalence of this respiratory pattern can help demystify its broader, long-term health implications and guide individuals toward appropriate diagnostic channels.
| Fact Category | Details |
| Symptoms |
|
| Causes |
|
| Types of Mouth Breathing |
|
| Age Group |
|
| You might be at a higher risk for exposure of this disease if you: 12 |
|
| How doctors diagnose |
|
| Other facts
13. |
|
How to Stop Mouth Breathing
Taking definitive control of your respiratory health begins with implementing targeted, evidence-based adjustments to both your daytime habits and nighttime routines. Transitioning safely from a dysfunctional oral pattern to a restorative nasal respiratory pattern requires addressing the physical blockages within your airway while simultaneously retraining the muscle memory that dictates your resting jaw posture.
1. Treat Underlying Nasal Congestion First
You must absolutely address any structural or inflammatory blockages within the nasal cavity before attempting to seal your lips. If your delicate nasal passages are severely swollen due to seasonal allergies, chronic rhinitis, or viral infections, forcing your mouth closed can lead to dangerous, intolerable drops in blood oxygen saturation. You should begin by utilizing highly effective conservative measures, such as hypertonic saline nasal rinses to physically flush out allergens, over-the-counter second-generation antihistamines, or prescribed intranasal corticosteroid sprays to calm mucosal inflammation 14. If major structural issues, such as a severely deviated septum or massive nasal polyps, are medically confirmed, you may need to consult an otorhinolaryngologist for definitive surgical correction.
Note: This foundational step is commonly used to rapidly decrease mucosal swelling, reduce overall airway resistance, and allow for comfortable, unforced nasal airflow.
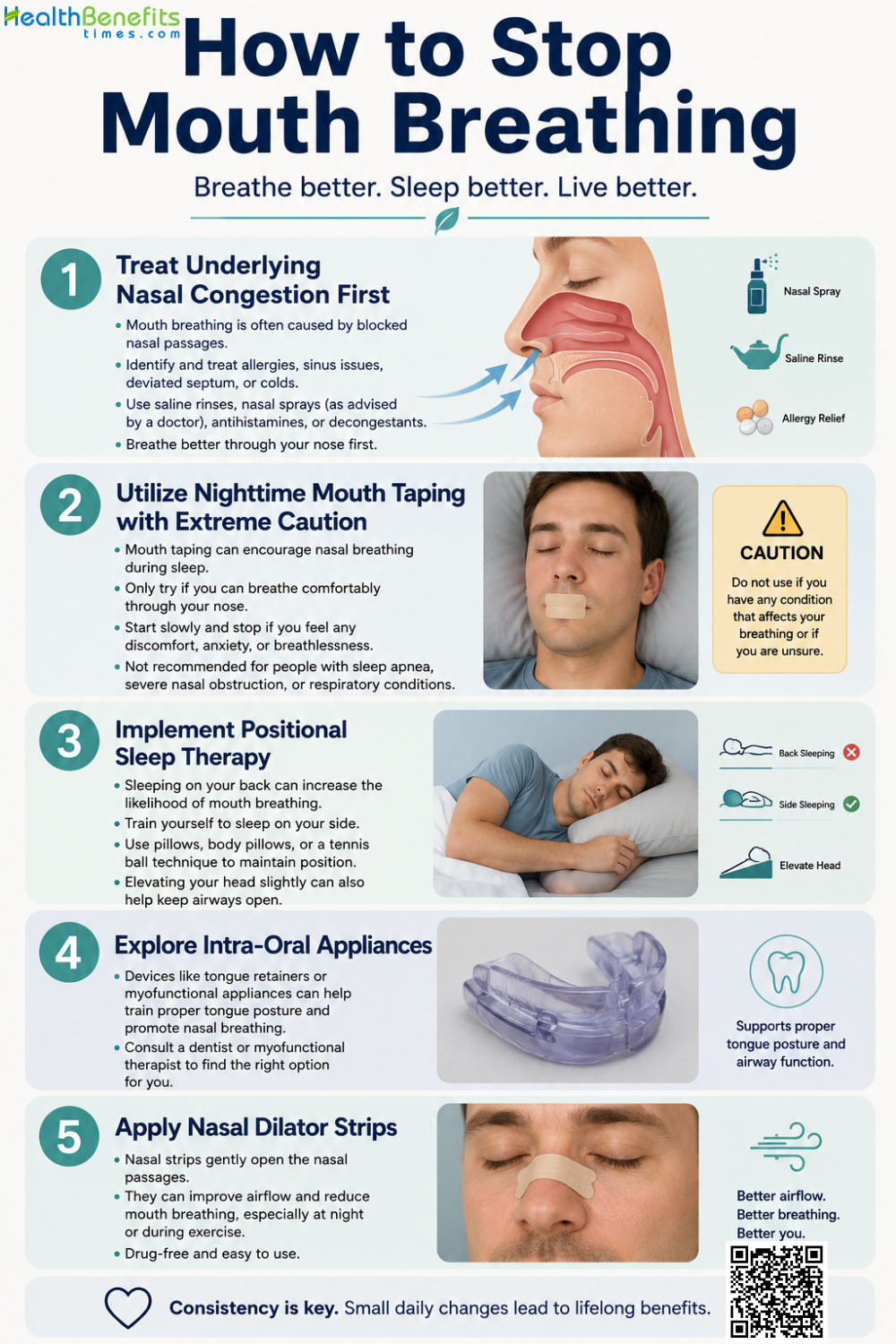
2. Utilize Nighttime Mouth Taping with Extreme Caution
Once your nasal passages have been clinically confirmed to be clear and fully patent, you might consider physical reminders to keep your jaw closed at night. You can apply a small strip of hypoallergenic, medical-grade porous tape vertically across the precise center of your lips immediately before sleep. This technique does not forcefully glue the mouth shut; rather, it serves as a gentle, continuous tactile cue that prompts your perioral muscles to maintain an active seal. However, you must exercise extreme, uncompromising caution: this method is strictly contraindicated and highly dangerous if you suffer from severe untreated obstructive sleep apnea (OSA), active chest infections, or acute nasal obstruction 15.
Note: This intervention is applied to physically maintain a lip seal during sleep and train subconscious neuromuscular memory, though it must be abandoned immediately if you wake up gasping for air.
3. Implement Positional Sleep Therapy
Adjusting your physical posture in bed provides another powerful, non-invasive tool to combat nighttime congestion and airway collapse. You should strictly avoid sleeping in a supine position (flat on your back), as the unyielding force of gravity naturally pulls the heavy base of the tongue and the soft palate downward, effectively crushing the pharyngeal airway. Furthermore, lying completely flat causes fluid and blood volume to pool directly in the nasal turbinates, exponentially increasing nasal airway resistance 16. You should elevate the head of your bed with a wedge pillow or utilize physical bumpers to train yourself to sleep exclusively on your side, utilizing gravity to keep the airway open.
Note: Positional therapy is commonly applied to prevent gravity-induced soft tissue airway collapse and reduce the localized hydrostatic fluid buildup that causes nocturnal nasal congestion.
4. Explore Intra-Oral Appliances
For more stubborn anatomical challenges or severe muscle flaccidity, you may need to rely on specialized dental hardware to stabilize your airway throughout the night. You can visit a qualified dental sleep specialist to be custom-fitted for a mandibular advancement device (MAD) or a specialized vestibular shield. These customized, precision-milled acrylic devices fit snugly over your upper and lower teeth and work by gently holding the lower jaw in a forward position. This anterior shift physically pulls the thick base of the tongue away from the back of the throat, widening the airway space 17.
Note: These devices are used for medicinal benefits to structurally stabilize the jaw, prevent the tongue from physically obstructing the airway, and mechanically enforce continuous nasal respiration.
5. Apply Nasal Dilator Strips
To ensure your nasal valves do not collapse under the negative pressure of inhalation, you can utilize external structural supports. You should apply over-the-counter, spring-loaded adhesive nasal dilator strips directly across the bridge of your nose before going to sleep. These strips physically lift and pull open the flexible cartilage of the lateral nasal walls, immediately expanding the cross-sectional area of the nasal airway and dramatically reducing the effort required to breathe through the nose 17.
Note: External dilators are applied for the immediate remedial benefit of physically widening the nasal airway to counteract the structural collapse of the nasal valves.
Is there any exercise or physical activities for Mouth Breathing?
Engaging the highly complex muscles of your face, mouth, and throat can dramatically retrain your body’s natural resting posture. Orofacial myofunctional therapy (OMT) acts as highly targeted physical therapy for your airway, helping to intensely tone flaccid muscles, correct improper swallowing mechanics, and establish a permanent, subconscious lip seal.
1. The Button-Pull Resistance Exercise
You can begin with simple, highly effective resistance training to strengthen your weakened perioral muscles, specifically targeting the orbicularis oris. You will need a large, smooth button (approximately 2 to 3 centimeters wide) and a strong piece of dental floss or string.
Note: How to do: Thread the string through the buttonholes, place the button directly behind your lips but in front of your teeth, and close your lips tightly around it. Pull the string gently outward away from your face while simultaneously using only your lip muscles to resist the pull and keep the button trapped inside your mouth. 18.
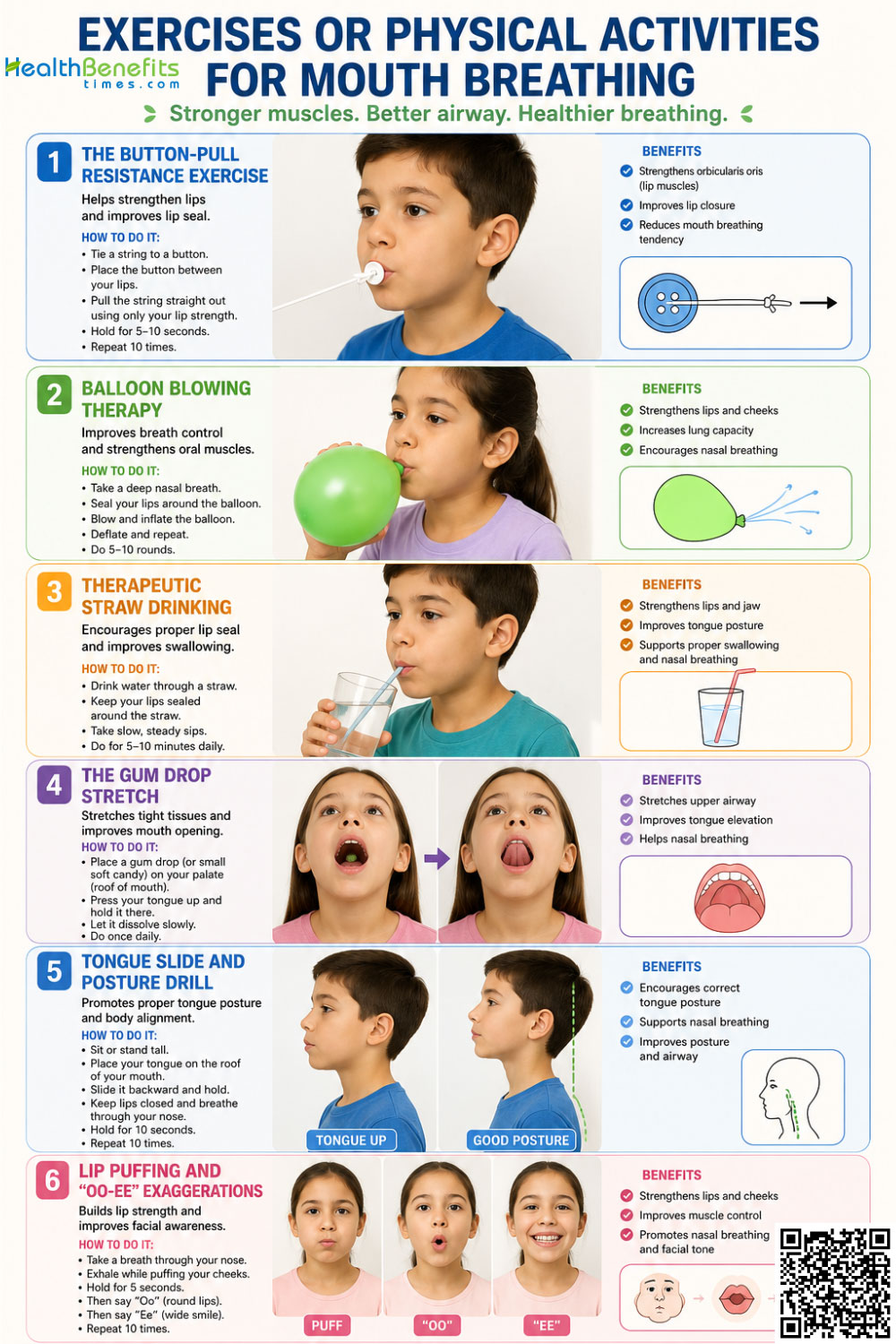
2. Balloon Blowing Therapy
Engaging the powerful diaphragm muscle while forcefully isolating the nasal airway provides a robust, systemic workout for the entire respiratory apparatus. You should keep a standard, high-resistance latex balloon handy for this daily breathing drill.
Note: How to do: Inhale deeply and exclusively through your nose, then place the balloon to your lips and exhale forcefully to expand it. Remove the balloon, close your lips immediately, inhale deeply through your nose again, and repeat the forced exhalation until the balloon is full. 18.
3. Therapeutic Straw Drinking
Repurposing everyday household items can yield surprisingly effective, high-resistance workouts for your oral cavity. You can replace standard open drinking cups with narrow, twisted straws, particularly when consuming thick, viscous liquids like smoothies, milkshakes, or yogurt.
Note: How to do: Place only a tiny, quarter-inch segment of a narrow straw between your lips and forcefully draw the thick liquid upward; the intense, sustained suction requires immense neuromuscular coordination and profound strengthening of the cheek and lip muscles.
4. The Gum Drop Stretch
Targeting and lengthening a short, hypertonic upper lip is vital if you suffer from lip incompetence (a structural inability to close the lips at rest without straining the chin muscles). You will need a heavy piece of candy, such as a large one-ounce gumdrop, securely tied to a piece of string.
Note: How to do: Place the free end of the string behind your upper front teeth and clamp down on it with your lips. Bend forward at the waist until your face is parallel to the floor, allowing the physical weight of the candy to dangle freely, and actively stretch your lips downward against the gravitational weight.
5. Tongue Slide and Posture Drill
Guiding your tongue into its correct anatomical home is perhaps the most critical step in this entire muscular retraining process. In a healthy, functionally mature resting posture, your entire tongue should be broadly suctioned against the roof of your mouth, not resting lazily on the bottom behind your lower teeth.
Note: How to do: Press the very tip of your tongue firmly against the alveolar ridge (the bumpy area of the palate just behind your top front teeth) and slowly slide the entire body of the tongue backward along the roof of your mouth as far as it will comfortably go, holding the intense upward tension for several seconds. 19.
6. Lip Puffing and “Oo-Ee” Exaggerations
Isolating the range of motion in your perioral area helps to establish independent muscle control, preventing the jaw from assisting the lips during closure. You should perform these rapid, exaggerated facial movements in front of a mirror to ensure symmetrical muscle engagement.
Note: How to do: Force a pocket of air directly between your closed lips and your front teeth, puffing out the lips as far as possible without letting the air escape. Follow this immediately by spreading your lips as wide as possible, then pursing them tightly, loudly articulating an exaggerated “oo-ee” sound.
Dietary and Lifestyle Adjustments
Navigating your daily environment successfully means keeping a highly watchful eye on dietary inputs and lifestyle triggers that might silently, progressively worsen your nasal congestion. Your delicate respiratory airway is highly reactive to both the complex chemical compounds in the foods you ingest and the physical demands you place on your body throughout the day.
Foods to Avoid When You Suffer from Mouth Breathing
1. Histamine-Rich Foods
You should pay exceptionally close attention to the underlying chemical composition of your daily meals, particularly regarding the presence of histamines. Histamine is a naturally occurring, highly potent biochemical compound that actively triggers the body’s inflammatory response, promoting heavy mucus production, tissue swelling, and vascular permeability in the respiratory tract. When you consume foods that have undergone extensive aging or bacterial action such as fermented vegetables (sauerkraut, kimchi), heavily aged and cured cheeses, smoked meats, and canned blue fish you introduce massive, overwhelming loads of exogenous dietary histamine directly into your systemic circulation 20. This sudden influx can rapidly worsen nasal congestion, swell the mucosal linings, and physically force you to abandon nasal breathing.

2. DAO Inhibitor Foods
Certain specialized enzymes located in your gut act as essential, natural defense mechanisms against dietary histamines, but consuming specific foods actively blocks this vital process. Diamine oxidase (DAO) is the primary metabolic enzyme responsible for breaking down and clearing histamine from your system. Foods and beverages such as strong citrus fruits (lemons, limes), pineapples, overly ripe bananas, heavily caffeinated black tea, and highly synthetic energy drinks actively inhibit your body’s natural DAO production 21. You should strictly restrict these items to prevent a dangerous metabolic bottleneck of histamines from inflaming your sinus cavities.
3. Alcoholic Beverages
You must be highly cautious and deliberate with alcohol consumption if you struggle with airway maintenance and snoring. Not only are many popular alcoholic drinks (especially red wine, champagne, and heavily fermented beer) inherently extremely high in raw histamines, but alcohol also acts as a profound, systemic central nervous system depressant and muscle relaxant 22. Consuming alcoholic beverages close to your intended bedtime unnaturally relaxes the pharyngeal constrictor muscles and the base of the tongue, virtually guaranteeing catastrophic airway collapse and heavy, strained oral breathing throughout the sleep cycle.
4. Excessive Refined Sugars
You should severely limit your daily intake of sugary snacks, candies, and highly processed carbohydrates. Chronic oral respiration severely dries out the protective saliva required to buffer and neutralize acidic plaque bacteria. Introducing a high-sugar, carbohydrate-heavy diet into a severely dry, unprotected oral environment creates a perfect, disastrous storm for rapid, severe dental caries and aggressive, painful gingival inflammation.
Activities to Avoid When You Suffer from Mouth Breathing
1. Sleeping in a Supine Position
Moving beyond the kitchen, your daily physical habits and environmental exposures dictate exactly how well your respiratory system functions at rest. You must actively avoid sleeping completely flat on your back in the supine position. As gravity relentlessly pulls fluids toward your head throughout the night, your highly vascular nasal turbinates swell with blood, and your relaxed tongue base collapses backward into the pharynx. This creates massive mechanical resistance that inevitably leads to jaw dropping, loud snoring, and forced oral breathing.

2. Exercising in Cold, Dry Air
You should also deeply reconsider your athletic environments and exertion levels if you are prone to respiratory distress and hyperreactivity. Engaging in prolonged, strenuous cardiovascular activities such as long-distance running, cross-country skiing, or intense cycling in freezing, highly arid climates forces massive volumes of unconditioned, raw air directly into your sensitive lungs 23. This severe thermal and osmotic shock can easily trigger exercise-induced bronchospasm, causing the lower airways to painfully constrict and further cementing the physiological need to gasp for air orally.
3. Neglecting Indoor Air Quality and Allergens
You should never neglect or underestimate the microscopic air quality of your immediate, enclosed living space. Allowing invisible dust mites to accumulate unchecked in heavy bedding, ignoring creeping mold in damp, poorly ventilated areas, or sleeping in the same room with heavily shedding pets will maintain a permanent state of chronic allergic rhinitis. You must actively launder all bedding in extremely hot water weekly and utilize high-efficiency HEPA air purifiers to keep your immediate breathing zone entirely free of mucosal irritants.
Myths and Misconceptions
Distinguishing scientifically proven fact from pervasive internet fiction is absolutely essential when exploring corrective therapies for respiratory disorders, as popular trends and anecdotal remedies often mask dangerous clinical realities.
| Myth | Reality |
| Mouth breathing directly causes enlarged tonsils and adenoids due to a lack of nitric oxide exposure. | Enlarged, hypertrophic tonsils and adenoids are typically the underlying root cause of the airway obstruction, not the downstream result of it. Objective clinical measurements routinely reveal that nitric oxide levels remain perfectly normal, or even slightly higher, in patients presenting with severely hypertrophic tonsils. |
| Mouth taping is a universally safe, simple, and guaranteed cure for all snoring and sleep issues. 25 | Blindly applying tape over the lips is highly dangerous and strictly contraindicated for individuals suffering from severe anatomical nasal obstructions, acute illnesses, or untreated Obstructive Sleep Apnea (OSA). It should absolutely never be attempted if the primary nasal airway is physically or structurally blocked. |
| Oral respiration is just a harmless, passing childhood habit that kids will eventually outgrow on their own. 9 | It is a highly complex, deeply destructive pathological adaptation. If left untreated during the early, rapid growth phases, chronic oral breathing can permanently alter the structural development of the facial skeleton, inevitably leading to severe malocclusion and a permanently constricted upper airway. |
| Breathing through the open mouth naturally gets larger volumes of oxygen to the brain than breathing through the nose. | Nasal respiration actually optimizes and maximizes cellular oxygen uptake. The paranasal cavity naturally produces nitric oxide, a vasodilator that travels to the lungs and increases systemic oxygen absorption by up to 18% compared to massive, inefficient oral respiration. |
Special Considerations
Every distinct stage of human life brings its own highly unique set of physiological vulnerabilities and complications when it comes to respiratory function and facial development. Tailoring effective interventions requires deeply understanding the specific anatomical, developmental, and hormonal landscapes of vastly different patient demographics.
1. Children
During the rapidly formative years of early childhood, the downstream consequences of improper breathing mechanics extend far beyond disrupted sleep and daytime crankiness. The human pediatric facial skeleton is highly malleable and heavily influenced by muscle pressure during early development. When a child chronically breathes through their mouth, the tongue drops to the floor of the mandible to allow air to pass, rather than resting firmly on the roof of the mouth. Without the constant, outward, structural pressure of the tongue to naturally widen and shape it, the upper jaw (maxilla) grows unusually narrow and high, inevitably leading to crowded teeth, severe overjets, and posterior crossbites 26. Furthermore, the severe lack of high-quality, restorative sleep resulting from chronic pediatric airway obstruction frequently manifests as clinical hyperactivity, poor academic performance, memory deficits, and irritability. These symptoms can tragically and easily be misdiagnosed as behavioral or psychiatric disorders, such as ADHD, rather than being correctly identified as a primary, correctable respiratory issue.
2. Pregnancy
Expectant mothers face an entirely different, heavily hormone-driven set of physiological challenges regarding their respiratory health. The dramatic, exponential surge in systemic estrogen and progesterone levels during gestation leads to vastly increased systemic blood volume and widespread, peripheral vasodilation. This profound hormonal shift frequently causes the delicate, highly vascular mucosal linings of the nasal passages to become severely engorged, swollen, and inflamed, a clinically recognized condition termed pregnancy rhinitis 27. As the nasal airway drastically narrows, pregnant women often reflexively resort to oral respiration to maintain air intake. This shift not only severely compromises maternal sleep quality and oxygenation but can theoretically reduce the vital partial pressure of oxygen transferred across the placenta to the developing fetus. This complex dynamic deeply underscores the critical, immediate need for safe, conservative, non-pharmacological management of maternal nasal congestion 28.
3. Chronic Conditions (Asthma and Allergies)
Individuals constantly battling long-term, chronic respiratory conditions often find themselves hopelessly trapped in a cyclical, self-perpetuating inflammatory loop. Under the medically accepted unified airway theory, the upper respiratory tract (nose and sinuses) and the lower respiratory tract (lungs and bronchi) function interdependently as a single, contiguous system. When chronic allergic rhinitis physically forces an asthmatic patient to abandon their nose and breathe orally, they entirely bypass the vital filtration, warming, and humidification processes provided by the nasal turbinates 29. Consequently, freezing cold, painfully dry, and highly allergen-laden air strikes the hyper-reactive bronchial tissues directly. This harsh, unconditioned insult severely promotes airway hyperresponsiveness, deeply aggravates lower airway inflammation, and can exponentially increase the frequency, duration, and severity of life-threatening asthma exacerbations.
4. Elderly
Aging populations routinely encounter unique anatomical breakdowns and functional declines that severely complicate maintaining optimal respiratory health. As individuals naturally age, baseline salivary gland function naturally and inevitably decreases, a phenomenon that is exceedingly often exacerbated by polypharmacy (the daily use of multiple prescription medications that list dry mouth as a side effect). When an elderly patient with already compromised salivary flow breathes heavily through their mouth throughout the night, the minimal remaining moisture in the oral cavity rapidly evaporates. This profound, chronic hyposalivation (xerostomia) brutally strips the fragile teeth of their protective, remineralizing salivary environment, dramatically accelerating rampant root decay, aggressive periodontal disease, and eventual complete tooth loss 30. Additionally, the natural age-related loss of firm muscle tone in the soft palate and pharynx massively increases the likelihood of catastrophic airway collapse, making nocturnal oral respiration a major, independent risk factor for the sudden development of late-onset obstructive sleep apnea and subsequent cardiovascular strain.
When to see a Doctor
Recognizing the crucial clinical boundary between a temporary, harmless head cold and a deeply entrenched, chronic respiratory disorder is absolutely crucial for protecting your long-term health, cardiovascular stability, and structural well-being. You should bypass home remedies and seek immediate, professional medical evaluation from an otorhinolaryngologist (ENT) or a certified sleep specialist if you or your child exhibit any of the following severe clinical warning signs:
- Persistent, Unyielding Daytime Fatigue: You experience crushing exhaustion, profound cognitive brain fog, frequent morning headaches, or an absolute inability to concentrate at work or school, despite seemingly spending an adequate eight hours in bed.
- Loud Snoring, Choking, and Gasping: You are repeatedly informed by a concerned sleep partner that you snore exceptionally loudly, emit choking sounds, or visibly and frighteningly stop breathing for several seconds during the night, all of which are textbook hallmark indicators of severe obstructive sleep apnea 31.
- Visible Craniofacial Changes in Children: You clearly notice a developing child habitually maintaining a perpetually open-mouthed resting posture, developing an elongated, narrow facial structure, or presenting with dark, swollen venous pooling (allergic shiners) under their eyes 32.
- Severe, Progressive Dental Malocclusion: You observe a rapid, unexplained shifting of teeth, an inability to bite into thin food with the front teeth (anterior open bite), or aggressive, bleeding gum inflammation that completely fails to resolve despite maintaining excellent daily brushing and flossing habits.
- Unresolved, Chronic Nasal Blockage: You suffer from a completely, structurally obstructed nasal airway that stubbornly refuses to respond to standard over-the-counter allergy medications, environmental controls, or hypertonic saline rinses over a continuous, multi-week period.
- Speech Impediments and Swallowing Difficulties: You or a child consistently struggle to cleanly articulate specific sibilant consonant sounds, possess a noticeable lisp, or frequently choke, gag, and rely heavily on copious liquids to successfully wash down solid food boluses during routine meals.